

Tonometry is the procedure for the measurement of intraocular pressure. It is the most important risk factor for the development and progression of glaucoma. It is the only factor that can be treated and modified in the management of glaucoma. Therefore, the need for accurate and reproducible measurement of IOP is of utmost importance.
Clinical measurement of IOP has undergone several technical advances from the initial digital tension measurements, through indentation tonometry, to applanation tonometry and non-contact tonometry.The current gold standard for the measurement of IOP is the Goldmann applanation tonometer.
Tonometer in which the IOP is negligibly raised during measurements, for example less than 5%, are termed low-displacement tonometer. Tonometer that displace a large volume of fluid and consequently raise IOP significantly are termed high-displacement tonometer.
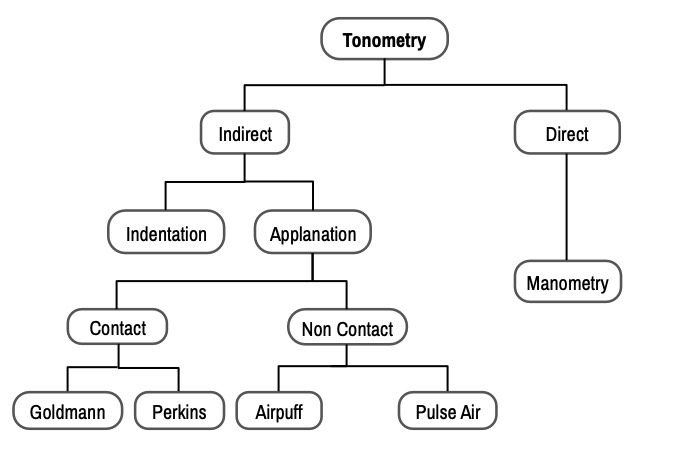
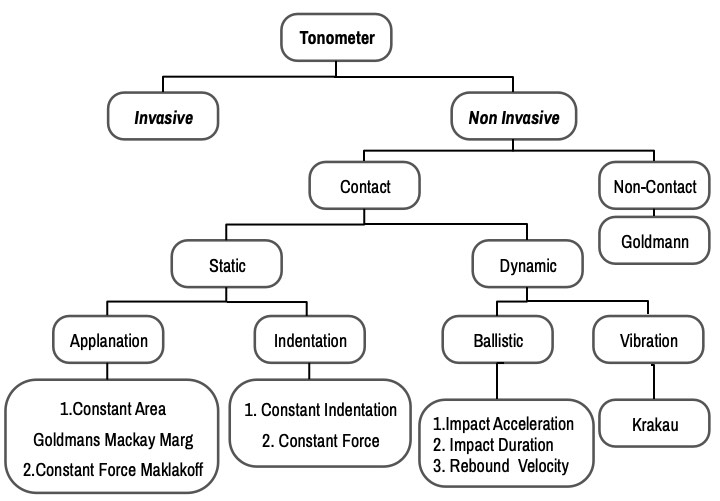
Classification and Types of Tonometers are shown in Flowcharts 1 & 2.
Difficulties in the Measurement of IOP
They mainly include
- Position of patient
- Inter & intraobserver variations
- Corneal surface abnormalities
- Corneal curvature
- Central corneal thickness
- Biomechanical properties of the cornea
- Corneal surgeries like kerato-refractive surgeries and intracorneal devices (e.g.INTACS)
1. Position of patient
IOP is higher in supine than in sitting posture due to increased episcleral pressure and probably due to the changed distribution of body fluids (thus yogic asanas like Sheershasana should be avoided by glaucoma patients). Thus, instruments measuring IOP in the supine position might record slightly higher readings than those in the sitting posture.
2. Inter & intraobserver variations
Most instruments have reasonably good reproducibility. However, GAT and Pascal Dynamic Contour Tonometer have been reported to have minimum inter & intraobserver variations.
3. Corneal surface abnormalities
Instruments that do not depend on optical systems like tonopen are more accurate for the measurement of IOP in corneas with ocular surface abnormalities or contact lenses.
4. Corneal curvature
The cornea with steeper curvature needs to be indented more requiring more force to produce a standard area of contact. The readings are affected more in DCT than in GAT.
5. Central corneal thickness
All forms of tonometry are affected by Central Corneal thickness. In general, higher CCT overestimates and lower CCT underestimates IOP. Dynamic contour tonometer and cornea compensated IOP measured by Ocular response analyzer are affected the least and Non-contact and Rebound tonometer readings are affected the most by CCT. Additionally, the thin central cornea is an independent risk factor for glaucoma progression.
6. Biomechanical properties of the cornea
The modulus of elasticity of cornea has been theoretically shown to have a greater effect on IOP measurement than either CCT or corneal curvature. Ocular Response Analyzer (ORA) is used to measure corneal hysteresis (CH) which reflects viscous properties.
7. Corneal surgeries
There is a decline in measured IOP following most of the keratorefractive surgeries including LASIK, LASEK, PRK, and even hyperopic LASIK and RK which cause minimal changes in CCT. There are further changes in recorded IOP as the wound heals postoperatively and probably reflects complex changes in biomechanics and elasticity of cornea following these surgeries. INTACS are mainly used to stabilize keratoconus or post LASIK ectasia. Such eyes have markedly altered biomechanical properties. Therefore, IOP in such eyes is better assessed (both pre and post-operatively) by devices less sensitive to altered corneal biomechanics like DCT or ORA. GAT and tonopen readings directly over INTACTS are shown to be unreliable than over central cornea.
Principles of Clinical Tonometry
Manometry, using intracameral cannulation, is the only method that precisely measures true IOP inside the eye. Being an invasive technique, it cannot be used in a clinical setting. Transpalpebral tonometry does not applanate or indent cornea. Thus, it bypasses inaccuracies related to scarring, edema, curvature, or biomechanical properties of cornea and sclera.
Types
Indentation Tonometer
- Plunger- to indent the cornea
- The shape of the deformation- truncated cone
- The significant volume of intraocular fluid displaced
Applanation Tonometer
- Force only to flatten the cornea
- Shape of deformation – simple flattening
Indentation Tonometers
Prototype – Schiotz tonometer, introduced in the year 1905
With the Schiotz tonometer, a series of known, standard weights are applied to the cornea via a plunger. The plunger indents the cornea, and a scale records the deformation of the globe. These two values are then used to determine the IOP. (Fig.1)
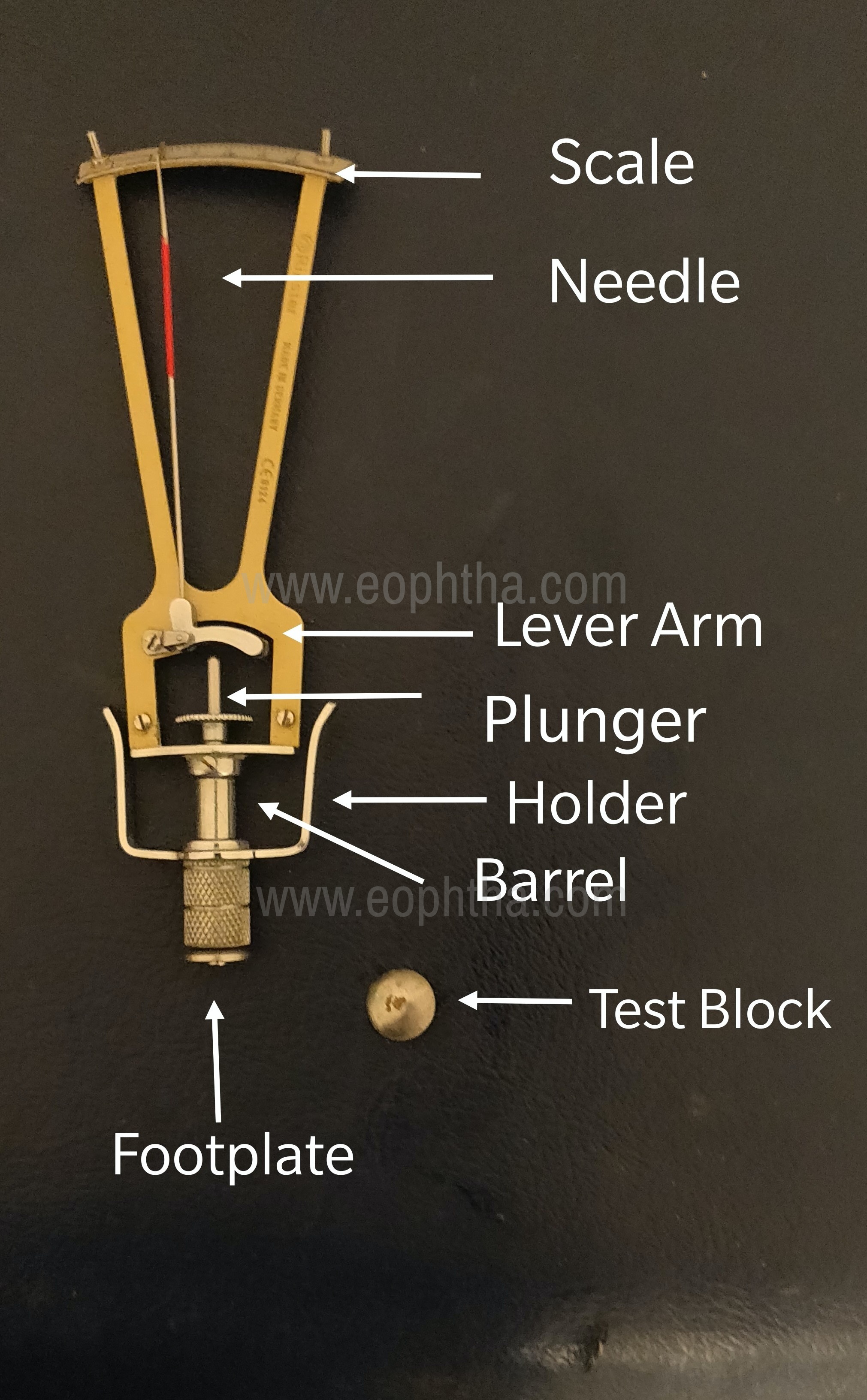
The plunger moves in a vertical fashion in the center of the instrument and passes through a curved footplate that sits on top of the cornea with the patient in the supine position. A “holder” fixes the footplate on the cornea but allows free movement of the plunger and the attached weights in the vertical direction. A movement of the plunger from its “0” position into the cornea can be correlated with the deformation of the cornea. Since the excursion of the plunger is relatively small and would be difficult to read, a lever magnifies the excursion along a more readable calibrated scale. When the tonometer is placed on the eye, the indentation of the cornea results in distention of the globe.
Friedenwald's formula relates this distention to the IOP. The formula required a constant “K” or the “coefficient of ocular rigidity,” which is a measure of the resistance of the eye to the distending forces of the tonometer. Presently, simplified tables exist that obviate the need for calculation and provide both the Po (pressure of undisturbed eye) and K values from the paired scale readings on the involved eye.
Procedure
The patient is supine with the cornea anesthetized. The patient is asked to fixate, tonometer footplate is applied to the cornea, the tonometer is kept vertical to allow free movement of the plunger to indent the cornea. The needle will oscillate with the ocular pulse, and the midpoint of the excursion is used as the scale reading. If the value is not greater than 4 units, additional weight is added. Then IOP read from the appropriate table.
Limitations
If the true K of the eye is higher than the average K, the table will overestimate the true IOP. Similarly, a false-low IOP will result if the true K is less than the average K.
False-high IOP readings
- thick corneas
- very steep corneas
- significant corneal pathology (irregular surface)
|
Low Ocular Rigidity |
|
|
|
Goldmann Applanation Tonometer
GAT remains the gold standard for routine ophthalmic practice.
Prototype: Goldmann Tonometer - Introduced in 1954.
Principle: Imbert-Fick Principle also referred as the Maklakov-Fick Law which says that for an ideal sphere (perfectly spherical, dry, infinitely thin walled and perfectly flexible), the pressure (P) inside sphere is equal to force (F)required to flatten/applanate the surface divided by the area (A) of flattening i.e. P=F/A.
Calculations: Since the cornea is not an ideal sphere, two other significant forces should be considered:
1. Force of capillary attraction (T) between tonometer head and tear film –additive to (F).
2. Additional force (C) independent of IOP is required to flatten the relatively inflexible cornea- opposite to (F).
Hence, F+T = PA+C i.e. IOP = (F+T-C)/A
‘A’ is located on the interior surface of the cornea.
Goldmann applanation is designed such that A=7.35 mm2 and diameter of flattening of the cornea is 3.06 mm. At this value of ‘A’, the opposing forces of capillary attraction and corneal inflexibility cancels out. In addition, at this ‘A’ the IOP (mmHg) = ten times the force applied to the cornea in grams, a convenient conversion. Since only 0.5μl is displaced from the eye and the pressure induced by the tonometer tip is negligible, applanation tonometry is not significantly affected by ocular rigidity.
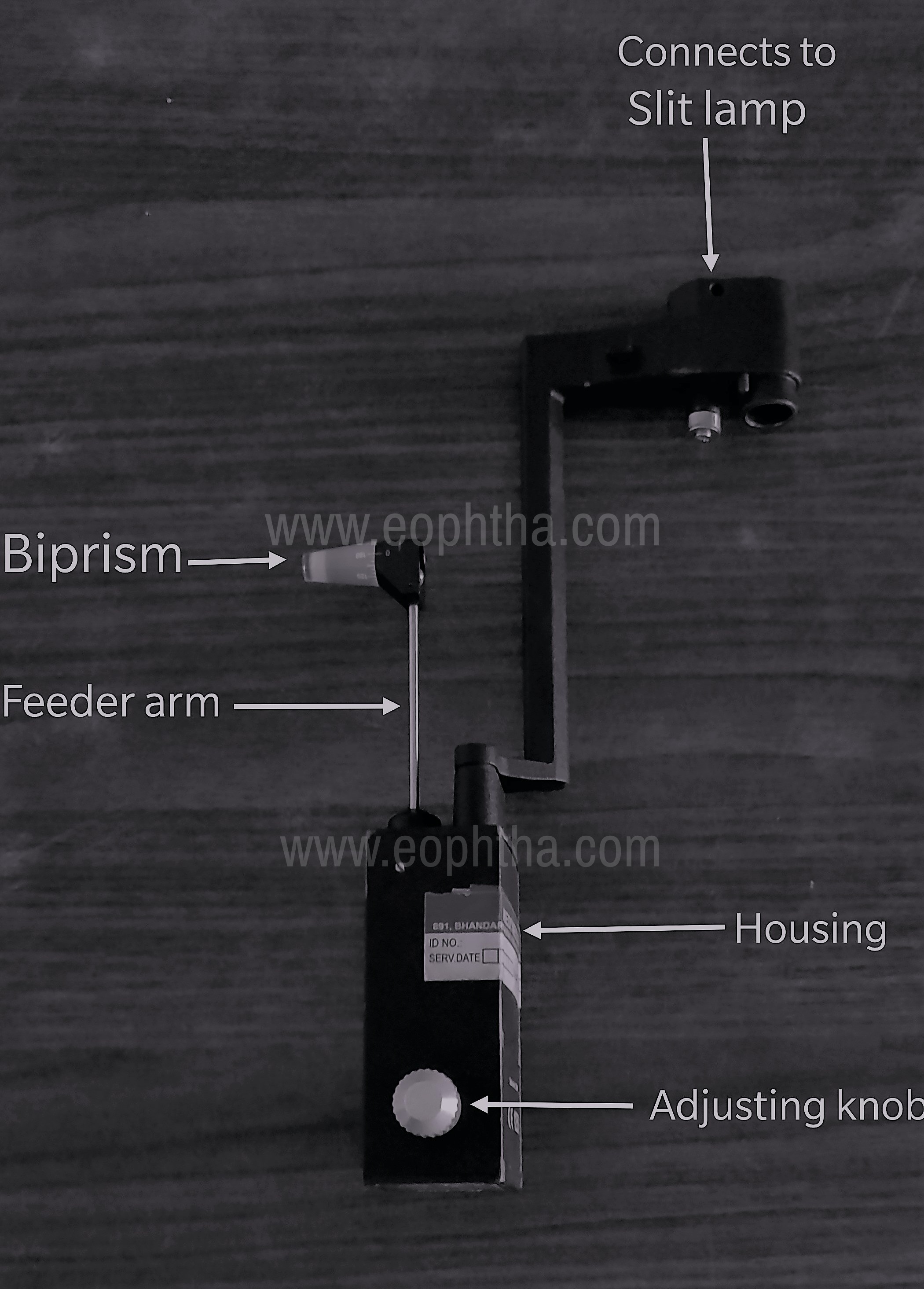
Instrument: The applanator tip contains a biprism which forms the contact point with the cornea. The tip is connected via a rod to the body of the tonometer, which contains an adjustable spring that provides the appropriate applanating force. The force is adjusted by a knob with a scale indicating the force applied in grams. (Fig.2)
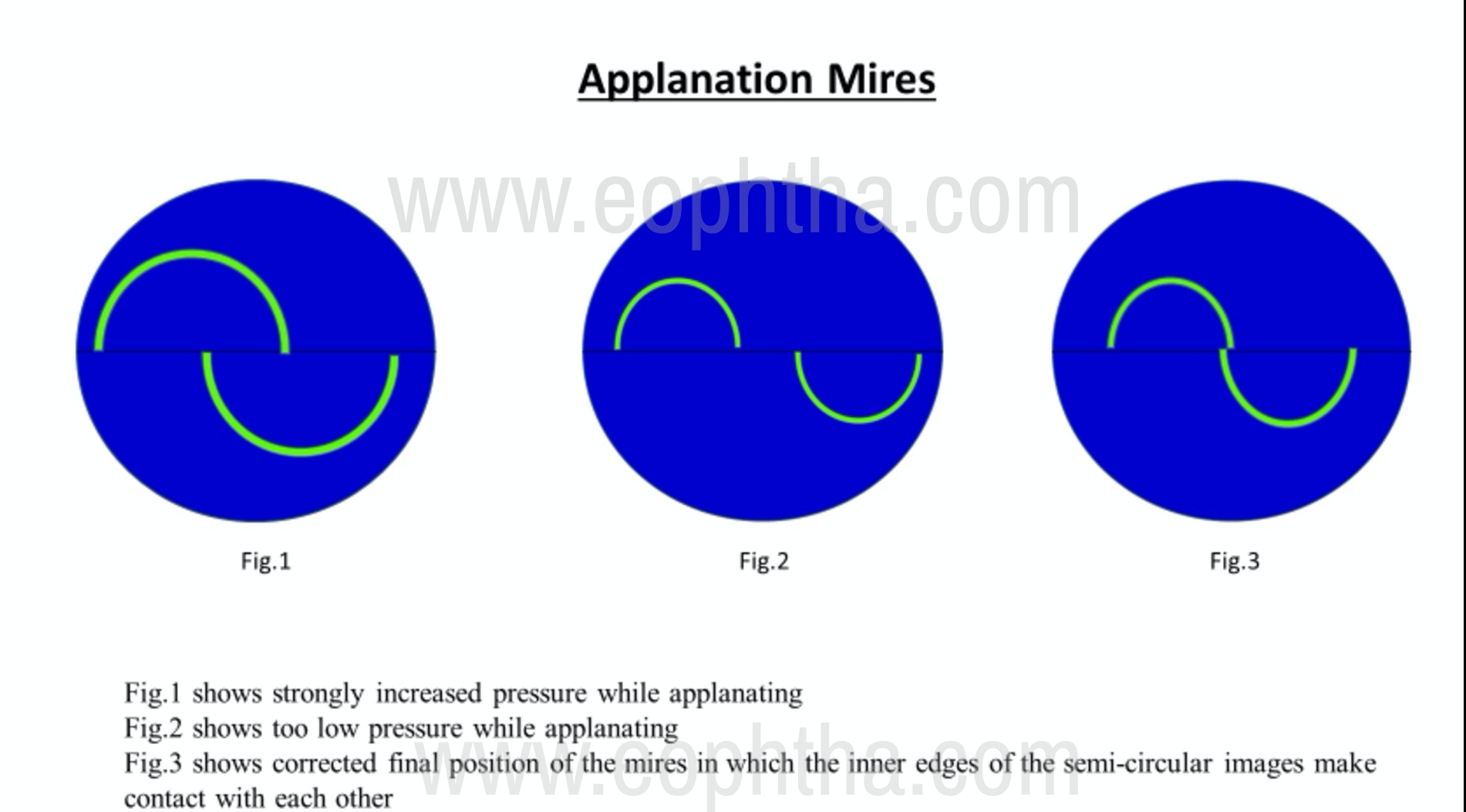
Clinical Measurement: The applanator is attached to slit-lampaligning the axis of the tip allowing visualization of the semicircles or mires. Maximum illumination with a cobalt blue filter is adjusted in the slit lamp. The patient is positioned at the slit lamp, the cornea is anesthetized and tear film is stained with 0.25% sodium fluorescein. The patient is instructed to fixate at distance, relax, and breathe normally. Breath-holding or Valsalva maneuver by patient should be avoided. The tip is advanced to approximate the cornea. The biprism splits the circle of contact into two semicircles/mires. When the inner margins of these semicircles touch, a 3.06 mm diameter circle of the cornea is applanated. The mires appear green against a blue background. If mires are unequal in size, vertical adjustments are made. The 1-gm position is used before each measurement. It is more accurate to increase rather than decrease the force of applanation. The tonometer knob is rotated until the endpoint is achieved. Ocular pulsations are noted and the internal margin of each mire is aligned. (Fig.3)
Sources of Error
1. Wide, blurred mires and vertical misalignment result in false high readings.
2. Corneal Variables: Thin corneas and corneas thickened by oedema produce false low IOP readings while thick corneas due to increased collagen result in false high readings. For every 3 dioptres increase in corneal power, the average IOP is increased by 1 mm Hg.
3. Corneal astigmatism results in a 1 mm error for every 4 dioptres, underestimating for with-the-rule and overestimating for against-the-rule astigmatism. To minimize this error, the biprism is rotated until the dividing line between the prisms is 45o to the major axis of the ellipse.
4. Prolonged contact with cornea gives false low IOP readings, apart from causing corneal injury.
5. Calibration should be done at least monthly.
Calibration
Calibration Position - (– 0.05): Rotate the measurement drum zero calibration downward by the width of one calibration mark. When the sensor arm is in the free movement zone, it should move against the stop in the examiner’s direction.
Calibration Position - (+ 0.05): Rotate the measurement drum zero calibration upward by the width of one calibration mark. When the sensor arm is in the free movement zone, it should move against the stop in the patient’s direction.
Other Applanation Tonometers
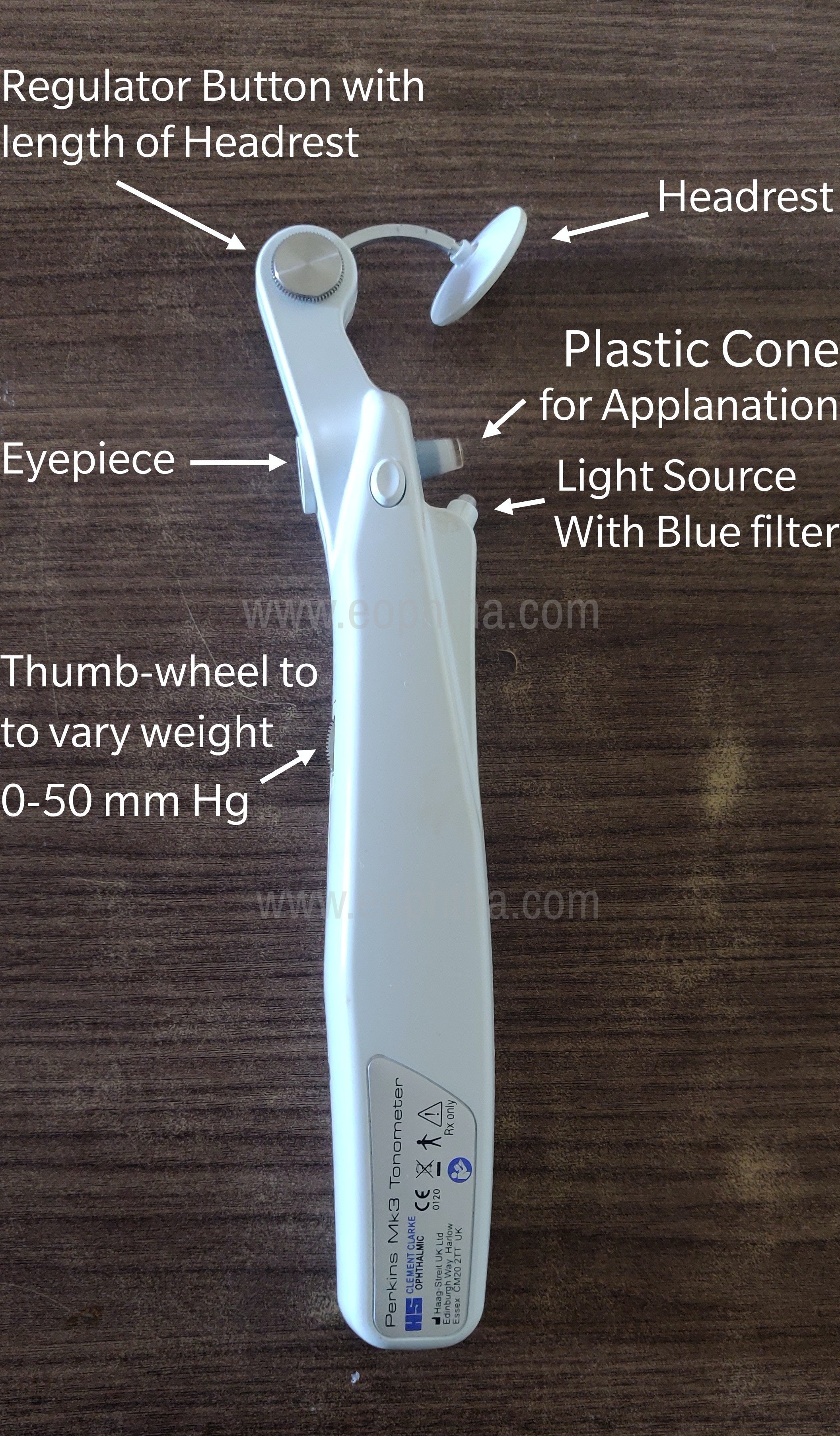
Perkins Applanation Tonometer
It is inaccurate on scarred, oedematous, or irregular corneas. Readings are consistent and comparable with the Goldmann applanator. It is a handheld tonometer especially useful for infants, children who cannot sit at the slit lamp. (Fig.4)
Draeger Applanation Tonometer
It is similar to the Goldmann and Perkins applanator except that a different biprism is used has an electric motor that varies the force. This instrument is also portable and useful in similar situations as the Perkins. It was introduced by J. Draeger (Germany) in 1966. This handheld tonometer weighs only 700gms.
Mackay Marg Tonometer
It is a new electronic applanation tonometer. It functions by applanating the cornea with a probe in the center of which is a small 1.5 mm diameter plunger that senses the ocular tension. The plunger is a fused quartz rod that moves through minute excursions. As the probe is gently pressed against the cornea, the plunger is depressed and the recording stylus traces a pressure curve. A typical curve shows an initial rise and a crest followed by a temporary trough and then rises; when the probe is removed from the cornea, the curve is retraced in a mirror image fashion. About less than half a second's applanation is sufficient to provide a good curve and usually, 4 to 5 applanations are done in each eye.
THE NEWER TONOMETERS
- Non-contact Tonometry
- Ocular Response Analyser
- Tonopen
- Pneumatic tonometer
- Dynamic Contour Tonometer – Pascal
- Rebound Tonometer
- Transpalpebral Tonometer
- Continuous IOP Monitoring Systems
- Diaton
1. Non-contact Tonometry
Mean IOP readings compare favorably with Goldmann tonometry, although relatively large discrepancies could be found in some patients. The instrument is beneficial in mass glaucoma screenings because it does not require topical anesthetic and, with proper use, there is no risk of injuring the cornea. (Fig.5)

Advantages
- Useful in screening programs
- Operable by non-medical personnel, user friendly
- No anesthesia required
Reported first by Grolman in 1972, it uses a jet of air to applanate anterior corneal surface. With the source of air in center, there is an optical system consisting of light emitter & detector on the two sides. As air-puff flattens the cornea, reflected light increases. The moment of applanation is the moment of maximal light detection by an optical sensor which shuts air pulse. The computer inside calculates IOP & displays it digitally. In the older machines, time from internal reference to the peak was converted to IOP whereas in newer machines, the IOP is measured from the actual air jet pressure required to applanate cornea.
2. Ocular Response Analyser (ORA -Reichert Corporation; USA)
Similar in principle to non-contact air puff tonometer, it measures the corneal response to indentation by a rapid air pulse. Precisely metered collimated air pulse causes cornea to move inward to applanate and even further into slight concavity. Then air pump shuts off. As the pressure decreases, cornea again passes through a second applanation state. Independent pressure values are derived from inward and outward applanation effects. Due to dynamic nature of air pulse and the viscoelastic properties of cornea the corneal damping causes delays in inward and outward applanation events resulting in two different pressure values. Average of two gives Goldmann correlated IOP (IOPg) & difference gives corneal hysteresis (CH). Cornea compensated IOP (IOPcc) utilizes information of individual corneal elasticity and viscosity. Thus, it measures not only IOP but also the deformability of cornea. ORA is used to measure corneal hysteresis (CH) which reflects viscous properties whereas corneal response factor (CRF) is calculated (P1- kP2, where k is a constant) and reflects elastic properties.
Corneal Hysteresis
CH is a measure of the viscous damping characteristics of corneal tissue. Measurement of CH has been proposed as an alternative to the gold standard, the Goldmann applanation tonometer. The approved indications are the measurement of intraocular pressure (IOP) and assessment of the biomechanical response of the cornea as tools in the diagnosing and monitoring of patients with glaucoma. Measurement of CH by the ORA has been proposed as a method to evaluate the potential for post-surgical complications in patients who are being considered for refractive surgery and for assessing the biomechanical properties of the cornea in keratoconus.
3. Tonopen
This is the portable version of Mackay Marg tonometer. In Mackay Marg tonometer, the force that is required to keep the flat plate of plunger flush with a surrounding sleeve against the pressure of corneal deformation is measured. The effect of corneal rigidity is transmitted to the sleeve. The IOP is recorded as wavefront. It is useful for irregular corneas as the area of applanation is small (1.5 mm diameter) and because it is not dependant on the optical system. This can give reasonably accurate readings over contact lenses as well. However, in band keratopathy, the surface is harder than the cornea and hence, it overestimates IOP. Tonopen uses an electronic gauge to flatten the cornea. The microprocessor inside averages several wavefronts and gives a digital display of IOP. An audible click is produced with a satisfactory wavefront. The IOP readings match well in the normal range. However, it gives higher values in eyes with low IOP and lowers values in eyes with high IOP when compared with GAT. As each IOP reading is taken over a brief period, it does not give any indication of the value around which IOP varies due to pulse & respiration and readings are affected by the cardiac cycle.
4. Pneumatic tonometer
It is similar in principle and recordings are similar to Mackay Marg tonometer. It applanates cornea with a probe that is supported by a column of gas and hence, the sensing device is air pressure. It is useful for diseased corneas, being non-optical. It can be used for continuous monitoring of IOP. It is different from the air-puff tonometer.
5. Dynamic Contour Tonometer – Pascal
Principle of Contour Matching
If eyes were enclosed by a contoured, tight-fitting shell, the forces generated by IOP would act on shell wall. Replacing a part of a shell wall with a pressure sensor would enable the measurement of these forces & therefore IOP. It was developed to eliminate errors inherent in previous tonometers, such as the effect of corneal thickness and rigidity, this instrument was made commercially available by Swiss Microtechnology® AG, Port, Switzerland (2002). The instrument is mounted on a slit lamp. The probe has a radius of curvature of 10.5 mm, contact surface of 7 mm diameter and sensor diameter of 1.2 mm. The PASCAL’s probe rests on the cornea with a constant force of one gram. Its piezoelectric sensor measures IOP 100 times per second with a resolution of 0.1mm. The plunger is concave and contour matched to the cornea and uses low appositional force thereby not causing any deformation of the globe while measuring the IOP. The instrument measures IOP in both diastolic and systolic phases of the cardiac cycle. The difference in the two is called ‘Ocular Pulse Amplitude’ (OPA) which is an indirect indicator of choroidal perfusion.
Display of DCT
The following are displayed on the LCD screen
- Diastolic IOP mmHg
- OPA mmHg
- Quality score- Score of 1 & 2 are satisfactory and 4 & 5 to be discarded. Manufacturers recommend the acceptance of score 3, most users feel it should be discarded.
Drawbacks of DCT
- More time consuming than GAT as 5 cardiac cycles need to be recorded.
- Doesn’t seem as useful in diseased corneas or after a corneal transplant.
- Tends to read a little higher than applanation tonometer in people with thin or average thickness corneas.
- Recurrent cost of disposable tip.
6. Rebound Tonometer
These are handheld ballistic devices that measure the return bounce motion of an object impacting the cornea. It is an electromechanical device consisting of two coils, a solenoid propelling and a sensing coil positioning around a central shaft containing a magnetized probe. The application of a transient electrical current to the solenoid coil propels probe to the cornea. This movement of the magnetized probe induces a voltage which is monitored by the sensor. On impact with the cornea, the probe decelerates and rebounds, and the microprocessor analyses deceleration of probe following the impact. This deceleration is less at low IOP than high IOP, thus, the higher the IOP, the shorter the duration of impact. With a diameter of 0.9 mm & weight of 26.5 mg, it is an easy to use instrument and no anesthesia is required, hence, it is useful in children too. However, CCT affects readings more than in GAT. On activation of the measurement button, it takes 6 readings and discards the highest and lowest readings on its own before giving a digital display of average IOP.
7. Transpalpebral Tonometer
Theoretically, these tonometers can overcome corneal problems like edema, astigmatism, variation in thickness, scleral rigidity, etc. But their accuracy is doubtful so has limited their use to self-tonometry by patients. E.g. TGDc-01and IGD-02 (2003) and Phosphene tonometer (1998). Phosphene tonometry is a psychophysical test for self-tonometry. The pencil-shaped instrument is pressed with its probe against the upper lid with increasing pressure until visual phenomena are detected. Phosphene appears opposite to pressure applied. Drawbacks include, patients with field loss may not perceive phosphenes.
8. Continuous IOP monitoring (Sensimed Triggerfish®)
Various tonometer can be used for continuous IOP monitoring. A recent addition to this list is SENSIMED Triggerfish which can be used for 24-hour IOP recording including sleeping hours. It uses a sensor which is a soft hydrophilic single-use contact lens, which has passive and active strain gauges embedded in the silicone to monitor fluctuations in the diameter of the corneoscleral junction. The output signal is sent wirelessly to the antenna, is directly correlated to fluctuations in intraocular pressure. The adhesive antenna, worn around the eye is connected to a portable recorder through a thin flexible Data Cable. The patient wears the contact lens up to 24 hours and assumes normal activities including sleep periods. When the patient returns to his doctor, the data is transferred from the recorder to the practitioner's computer via Bluetooth technology for immediate analysis. Although considered a breakthrough solution to continuously monitor fluctuations of intraocular pressure by the manufacturer, the cost is prohibitive.
9. Diaton Tonometer
It is portable and handheld, the Diaton does not require sterilization or anesthesia. Because it measures IOP through the eyelid over the sclera, it is not affected by central corneal thickness or corneal rigidity.
Tonometry in Paediatric Patients
1. Perkins Tonometer
The Perkins applanation tonometer is similar to the Goldmann applanation tonometer except that it is portable. This handheld device allows for measuring IOP in both the upright and supine positions. Therefore, the Perkins applanation tonometer is ideal for examining babies, children, uncooperative patients, wheelchair-bound patients, and bedridden patients as well as during an examination under anesthesia (EUA)
2. Tono-Pen applanation tonometry
The Tono-Pen is a portable electronic applanation device that applanates a small area of the cornea using batteries for power. This device is particularly useful with corneal scars or edema. Because it is portable, it is useful in the office setting as well as during a EUA.
3. Pneumotonometry
The pneumotonometer is a pressure-sensing device and is particularly useful for patients with corneal scars or corneal edema.
Icare® (rebound tonometry)
The rebound tonometer is a handheld portable instrument with distinct advantages for the pediatric population. Because the light-weight probe makes only momentary contact with the cornea (i.e., 0.25 to 0.30 meters/seconds), its main advantage is that topical anesthesia is not required. It is particularly useful in children who do not tolerate Goldmann applanation tonometry and in situations where repeated EUAs may not be advisable because of the health and safety concerns of repeated anesthetic exposure for children younger than 3 years. It has also been used in home settings, in situations when patients are unable to follow-up for frequent IOP assessments and to monitor diurnal variations.
Sterilization
The prisms which touch the cornea need to be sterilized appropriately to prevent cross infections (Goldmann, Perkins, Draegers, and Pneumotonometers). Mackay-Marg and Tonopens have sterile tonofilm covers.
The methods to sterilize tonometer prisms include:
1. Disposable mechanical wipe and sterile gauze. (does not protect against HSV 1 and 2)
2. Wipes soaked (or pre-soaked) in 70% isopropyl alcohol or 3% hydrogen peroxide.
3. Soaking the tip of the prism in 70% isopropyl alcohol, 3% hydrogen peroxide, or 1:10 household bleach.
4. Ultraviolet rays.
5. Gas sterilization.
Tonometry in Special Situations
|
1. |
Irregular corneas |
Pneumatic Tonometer, Mackay Marg, Tono-Pen, DCT |
|
2. |
Over soft Contact Lenses |
Pneumatic Tonometer and Tonopen |
|
3. |
In Gas-Filled eyes |
Pneumatic Tonometer and Tonopen |
|
4. |
Post LASIK status |
DCT |
|
5. |
Children/Screening programs |
Perkins, NCT, I- Care |
References
- Shields Textbook of Glaucoma 6th edition
- Becker-Shaffer’s Diagnosis and Therapy of the Glaucomas 7th edition
- Singh M.D. Newer Tonometers. DOS Times. 2011; 16(9): 57-63
- Sood D, Honavar S G. Sterilisation of tonometers and gonioscopes. Indian J Ophthalmol 1998;46:113-6
- American Academy of Ophthalmology https://www.aao.org/eyenet/academy-live/detail/goldmann-tonometer-remains-gold-standard-iop