
Introduction
Dystonia is defined as a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal, often repetitive, movements, postures, or both [1]. They may be isolated or combined with other neurological symptoms or movement disorders [1]. Dystonia is classified based on the age of onset, etiology, clinical features, and body distribution. The body distribution may be either focal, segmental, multifocal, generalized, or hemi-dystonia. Only one region of the body is affected by focal dystonia. It emerges in late adulthood [1].
Patients with movement disorders isolated to the facial region often visit an Ophthalmologist. A brief knowledge about the identification and differentiation of the various facial movement disorders is essential. The disorder can be functionally or socially distressing to the patients.
The facial movement disorders include orbicularis myokymia, Benign Essential Blepharospasm (BEB), Apraxia of Lid Opening (ALO), Hemifacial spasm, Meige’s syndrome, and aberrant regeneration of facial nerve [2-6].
Pathogenesis
A basic idea of the blink reflex will help understand etiopathogenesis.
The blink reflex:
- Generated by stimulation of the supraorbital area, conjunctiva, or cornea
- Afferent branch: Ophthalmic branch of the trigeminal nerve
Supraorbital skin: supraorbital nerve
Cornea and conjunctiva: Long ciliary nerve
- Sensory nucleus of trigeminal projects to the motor nucleus of the facial nerve
- Efferent branch: Motor branches of the facial nerve – Zygomatic, buccal, temporal
Components:
Early and late blink reflex
- Early
- (ipsilateral) oligosynaptic arc in the pons
- supraorbital sensory trigeminal root to the ipsilateral facial nucleus
- Late blink reflex and corneal reflex
- (bilateral) polysynaptic pathways in lateral reticular formation in the lower brainstem (pons and medulla)
- descending spinal fifth nerve nucleus to ipsilateral and contralateral facial nucleus
The supranuclear and cortical control of blinking and eyelid movements is not very well understood. It is thought that the basal ganglia are the central control center. Movement disorders occur secondary to disturbance or damage in this circuit [4-6].
Orbicularis Myokymia
Transient involuntary, continuous fine contractions, most commonly affecting the lower eyelid (Video 1). It is usually unilateral and lasts from few days to weeks. The contractions can occur intermittently through the day lasting up to a few hours at a time [2].
Orbicularis myokymia occurs in the setting of stress, anxiety, excess caffeine intake, or physical exertion [2]. Rarely it has been reported secondary to drugs such as topiramate, clozapine, gold salts, and flunarizine [3].
Treatment
Condition is usually self-limiting. Adequate rest helps. The offending drug can be discontinued in case of drug-induced myokymia. Botulinum toxin injection can be given in cases where the patient is affected by the contractions [2-4], [6].
Benign Essential Blepharospasm
Blepharospasm is a type of focal dystonia caused by dystonic contractions of the orbicularis oculi, procerus, and corrugator supercilii muscles. The onset is between the 5th to 7th decade with a female preponderance [4], [5].
Increased risk of developing Benign Essential Blepharospasm (BEB) has been noted in psychiatric patients and in those with a stressful lifestyle [5]. Up to a third of patients have a positive family history with an autosomal dominant inheritance pattern with reduced penetrance. Genes implicated in its development include GNAL, CIZ1, TOR1A, DRD5, and REEP4 [5]. Dry eye is associated with about 60% of patients and photophobia in up to 80% of patients [5], [6].
BEB should be differentiated from secondary blepharospasm which is caused by ocular surface disorders like dry eyes, keratitis, etc., or irritation in the supraorbital area.
In BEB, there is a disorder in the primary blink reflex mechanism wherein an increased supranuclear input results in increased amplitude and duration of blink response. Lesions such as stroke in the thalamus, cerebellum, midbrain, lower brainstem, basal ganglia, substantia nigra, and dentate nucleus can have blepharospasm as one of the features along with other neurological manifestations [6].
Charcot sign [6]:
- Lowering of brows below the superior orbital rim. Indicates intense contraction of the orbital part of orbicularis.
- Useful to differentiate from apraxia of eyelid opening.
Grading systems [6]:
- Jankovic rating scale: A 5-point grading system that includes a severity score and a frequency score (Table 1).
- Blepharospasm severity scale: Consists of 6 clinical items-
- Degree of eyelid closure
- Duration of closure
- Frequency of spasm
- Blink rate
- Apraxia of eyelid opening
- Lower face spasms
|
JRS severity |
|
|
0 |
No symptoms |
|
1 |
Increased blinking produced only by the action of external stimuli (e.g. bright light, wind, reading, etc.) |
|
2 |
Mild, spontaneous blinking (without spasms), clearly visible, sometimes troublesome, but with no functional impairment |
|
3 |
Moderate, clearly visible spasms of the eyelids; moderate impairment |
|
4 |
Severe, impairing spasms of the eyelids, probably with involvement of other facial muscles |
|
JRS frequency |
|
|
0 |
No symptoms |
|
1 |
Slightly increasing blinking frequency |
|
2 |
Flickering of eyes with individual blink duration of less than one second |
|
3 |
Spasms of the eyelids lasting more than one second; eyes open more than 50% of waking time |
|
4 |
Functional blindness caused by the prolonged closure of the eyes for more than 50% of waking time |
Table 1: Jankovic rating scale (JRS)
Management
Investigations:
No neuro-imaging is necessary unless BEB is associated with other neurological manifestations. Electromyography in BEB shows the presence of R2 blink response with stimuli delivered at small intervals of 100-200ms. This is useful to rule out psychogenic dystonia [5].
Treatment:
Using photochromatic glasses (FL-41 lens tint) reduces photophobia.
Chemodenervation with Botulinum toxin is the first-line treatment. The injection sites are as shown in Figure 1. About 2.5-5U is injected at each site.

Figure 1: Standard injection sites for Benign Essential Blepharospasm. Upper eyelid, above the punctum, pre-tarsal (1), upper eyelid, above the lateral canthus, pre-tarsal (2), lower eyelid, below the punctum, pre-tarsal (3), lower eyelid, below the canthus, pre-tarsal (4). Lateral canthal: 1cm lateral to lateral canthus (5). Brow injections: 8mm above the brow, at the junction of the medial and middle third (6), at the junction of the middle and lateral third (7). Eyelid injections are subcutaneous, and brow injections are deep. Additional brow sites, procerus, and lower facial muscles (Meige’s syndrome) can be customized as per need. Prior application of Lidocaine-Prilocaine topical anesthetic cream reduces pain while injection.
Clinical response is seen in about 2-3 days. The effect lasts for about 2-4 months following which the injection needs to be repeated [5], [6].
Oral Pharmacotherapy:
Oral medications like benzodiazepines, anticholinergics, lithium, etc. have a limited role in BEB. Moreover, they are associated with systemic side effects and risk of dependence. However, they may be considered in refractory BEB keeping in mind the suboptimal response [5], [6].
Surgical intervention
Subtotal and total orbicularis myomectomy can be performed in refractory cases (Figure 2) [5], [6].

Figure 2: Orbicularis myectomy for BEB. In limited myectomy, an eyelid crease incision is taken to remove the pre-tarsal and pre-septal orbicularis oculi muscle. The muscle is separated from the skin above, and the septum below, and excised. In extended myectomy, the orbital part of the orbicularis, corrugator, and procerus are also removed.
Other treatment modalities have also been described-
- Chemodenervation with doxorubicin injection
- Differential section of seventh cranial nerve (facial nerve) in patients with failed myectomy (21%). The zygomatic branch is targeted for ablation. The procedure is successful in up to 75% of patients but has a high complication rate which includes paralytic ectropion, brow ptosis, lip paresis, and ptosis of the angle of the mouth[4-6].
Apraxia of Lid opening
First described by Goldstein and Cogan, Apraxia of Lid Opening (ALO) is difficulty in opening eyelids voluntarily. This abnormality can be associated with extrapyramidal disorders particularly progressive supranuclear palsy [4]. The peak onset is at the 6th decade with female preponderance. Overactivity of pretarsal orbicularis along with failure to initiate or sustain LPS activity during eyelid closure is understood to cause ALO (Figure 3).

Figure 3: Apraxia of Lid Opening. A 57-year-old man with the inability to quickly open the eyes upon volitional closure (a). he struggles for 4-8 seconds before he can open his eyes (b). Pre-tarsal orbicularis oculi muscle is targeted with 4 sites of injection, and 10 units of Botulinum toxin per eyelid (c). Same patient with considerably reduced lag in opening the eyes 2 weeks post-injection (d).
ALO associated with BEB is not true apraxia. It is a focal dystonia of eyelids also termed pretarsal blepharospasm.
Differentiation from BEB [6]:
- The absence of Charcot sign helps in differentiating it from BEB. There is an elevation of brows secondary to frontalis overaction in an attempt to lift the eyes open.6
- Chin up position, reduction in periodic blinking, and lack of photophobia are often present.
- BEB and ALO can often co-exist.
Treatment
Botulinum toxin is given in the pretarsal orbicularis (2.5-5 U) and surgery reserved for refractory cases. Crutch glasses help and Frontalis suspension can be performed to aid in the mechanical opening of the eye.
Hemi-facial spasm
Hemi-facial spasm (HFS) is a movement disorder wherein there is involuntary, irregular, tonic, and clonic synchronous contraction of the muscles innervated by the ipsilateral facial nerve (Figure 4). The onset is between 4th and 5th decade with female preponderance [4]. The initial site is the orbicularis muscle in 90% cases followed by the cheek (11%) and perioral region (<10%). The contractions begin in the peri-ocular region and gradually spread over the cheek and perioral region over months to years. About 1.2-2.6% of patients may have bilateral HFS.

Figure 4: A 51-year-old lady with left Hemifacial spasm of 3 years duration (a). Note the active downward movement of the brow, contracture of the orbicularis oculi, upward movement of the left angle of the mouth due to contraction of the zygomaticus major, chin puckering due to mentalis, and contracture of the platysmal band over the left side of the neck. Two weeks following 15 units of Botulinum toxin injection, her spasm frequency reduced considerably (b).
Vascular compression of the facial nerve root exit zone in the subarachnoid space in the posterior fossa causes Primary HFS. An aberrant loop of anterior (43-60%) or posterior inferior cerebellar artery (28-31%), vertebral artery or basilar artery (12-23%), or a venous aberrant loop can compress. The compression may lead to stretching, bending or demyelination of nerves in addition to the pulsatile nature causing neuropathy [4], [6].
Secondary HFS is due to other causes like cerebropontine tumors, arachoid cyst, arteriovenous malformations, or other brainstem lesions [4], [6].
Based on the vessels causing compression, HFS can be classified as [6]:
- Type 1 – AICA type (Anterior inferior cerebellar artery)
- Type 2- PICA type (Posterior inferior cerebellar artery)
- Type 3- VA type (Vertebral artery)
Clinical differentiation from BEB [6]:
- Presence of spasms during sleep (due to pulsatile vascular compression on the nerve)
- Babinski-2 sign: During eye closure when orbicular contracts, the medial part of the frontalis also contracts to raise the brow. Abnormal facial nerve activity results in synchronous orbicularis and frontalis muscle function.
Management
Investigations:
MRI brain imaging is recommended to rule out any intracranial pathology with special attention to the area of the pontomedullary sulcus. High-resolution thin section T2 weighted MRI images nerves and vessels. For assessment of small arteries, CTA (Computed tomography with angiography) is useful. It is important to communicate with the Radiologist before requisition to look for the suspected pathology [4], [6].
Treatment
1. Microvascular decompression surgery
This involves neuro-surgical intervention wherein the compressive vascular loops are placed away from the nerve in this surgery. The success rates are between 84-98%. Complications include ipsilateral hearing loss, facial nerve weakness, and brain-stem infarction [4], [6].
2. Botulinum toxin injections
There is good functional and clinical outcome with botulinum toxin injection. The sites of injection are as shown in figure 5. Due to temporary action, the injections must be repeated every 3-6 months.
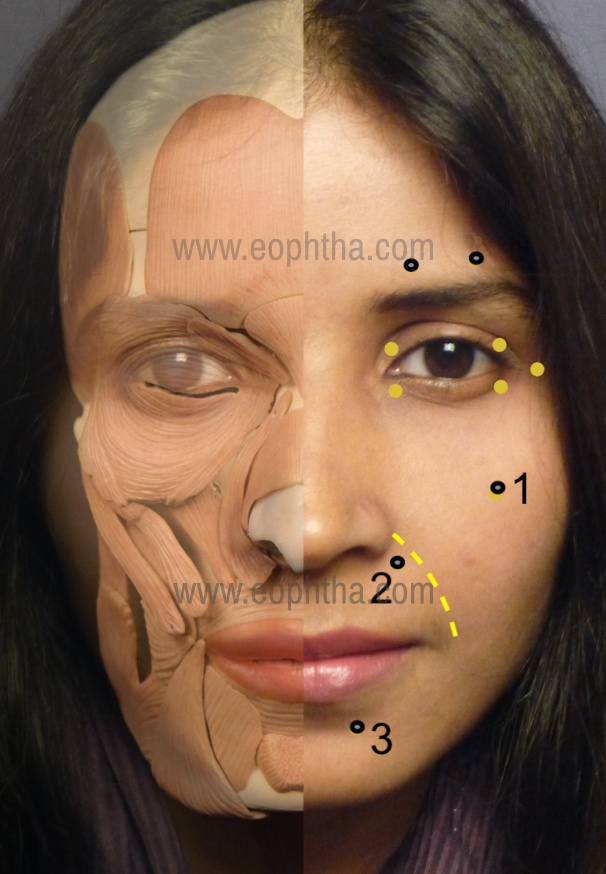
Figure 5: Standard injection sites for Hemifacial spasm. The eyelid and brow sites remain the same as that for BEB. Additional sites are as follows. Zygomaticus major: The origin of the muscle is palpated just under the prominence of the zygoma, to inject deep (1). The levator labi superioris alaeque nasi is responsible for the upward twitch of the lip and is targeted infero-medial to the nasolabial fold (dotted line) where it lies just below the skin (2). The mentalis muscle is targeted in the chin if the chin puckering is objectionable (3). Many patients prefer bilateral treatment for symmetry of smile and blink.
3. Oral medications
The response is poor to oral medications. Phenytoin and carbamazepine have been tried with limited success.
Meige’s syndrome
Meige’s syndrome is a segmental (craniocervical) dystonia characterized by the presence of oromandibular and cervical dystonia and blepharospasm. Though the condition was described by Henry Meige in 1910, George Paulson named it “Meige’ syndrome [7]. The onset is between 30-70 years of age with a female predilection.
Clinically, the spasms begin as unilateral or bilateral blepharospasm and later spread to other muscles of the jaw and neck. It can spread to the muscles of the upper limb or respiratory muscles. The spread occurs over 3-5 years. Grimacing, lip pursing, chewing, clenching, jaw thrusting, and opening are some of the facial movements seen in these patients [6], [7].
Female gender, older age of onset, history of head trauma, blepharospasm are some of the risk factors for the spread of these movements [7]. These patients also have sensory tics to attenuate dystonia like yawning, sleeping, humming, drinking, talking, walking, pulling the upper eyelid, etc [4], [6].
Meige syndrome should be differentiated from Brueghel syndrome, in which is only jaw dystonia is noted with no blepharospasm [7].
Primary Meige syndrome
Certain genetic mutations have been identified to be the underlying cause of Meige syndrome, these include- GNAL (gene for guanine nucleotide-binding protein G, subunit alpha) and p.Gly213Ser / p.Ala353thr [6], [7].
Secondary Meige syndrome
Facial and cervical dystonia secondary to long-term use of neuroleptic drugs, head trauma, stroke, encephalitis. Neuroleptic drugs alter the receptor function alteration resulting in denervation hypersensitivity. The increased central dopaminergic activity also causes dystonia.
It can be associated with other movement disorders like Parkinson's disease, Wilson disease, etc [6], [7].
Management
Investigations:
Systemic workup is warranted in cases with clinical suspicion of secondary Meige syndrome. MRI or CT brain to rule out intracranial pathology or stroke.
Treatment [6], [7]:
1.Oral pharmacotherapy:
Anticholinergics, dopamine antagonists, GABA receptor agonists, antiepileptics are effective.
2. Botulinum toxin injection
Considered in cases of poor response to oral medications. The periocular injection sites are similar ot that of BEB. Additional lower facial injections can be given as per the muscles involved.
3. Deep brain stimulation of the globus pallidus interna may be effective in select patients with limited response to oral medications and botulinum toxin.
Others
Aberrant regeneration of facial nerve
Synkinesis due to aberrant facial nerve regeneration is not a dystonic disorder but a muscle movement disorder due to abnormal nerve connections. Involuntary movement following a voluntary movement by a muscle group is termed synkinesis [6]. It is one of the sequelae of incomplete facial nerve paralysis apart from facial muscle weakness, asymmetry, atrophy, and hyperkinesis. About one-third to half of facial nerve palsy patients have been reported to have incomplete recovery of facial nerve function [8].
Ineffective myelination, hypersensitization of nerve fibers during the process of regeneration results in synkinesis. There is an abnormal connection between the lower fibers of the facial nerve with those supplying the orbicularis.
The classification is based on the groups of muscle involved in the voluntary-involuntary movement i.e oculo-oral or ocular-oral synkinesis. In other words, on voluntary eye closure, there is involuntary twitching around the lips and voluntary lip movements are followed by decreased palpebral fissure or twitching around the eyes [6].
Others include gustatory hyperlacrimation (unilateral lacrimation on eating), platysma, and mentalis contraction.
Clinically, there is facial asymmetry, hyperactivity, prominent platysma, deep nasolabial groove, eyebrow elevation, hyperlacrimation, poor smile mechanism [6]. With oral movements, there is a narrowing of palpebral fissure height (Figure 6).
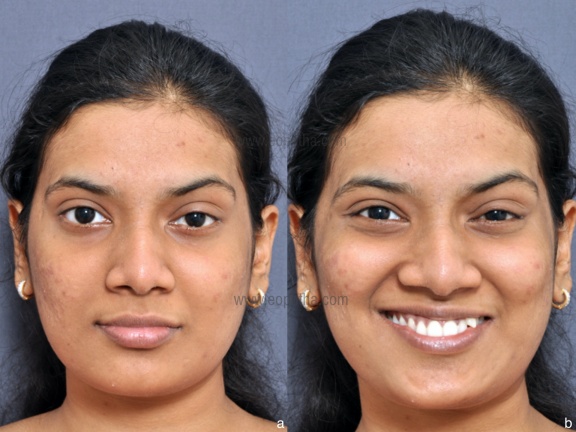
Figure 6: A 23-year-old girl with recovered Bells palsy (a), showing the reduction in the left palpebral fissure height during the act of smiling (b). Note the slightly weak action of zygomaticus major on the left. Botulinum toxin injections in the periocular orbicularis can improve this cosmetic deformity caused by co-contraction of zygomaticus major and orbicularis oculi.
Differentiation from Marcus Gunn Jaw-wink syndrome:
Excursion of the upper eyelid with Jaw movements. There is abnormal innervation between trigeminal (muscles of mastication) and oculomotor nerve (levator palpebrae superioris). So, with jaw movements, the palpebral fissure height widens [6].
Management:
Investigations:Not warranted
Treatment:
1.Exercise therapy
Facial exercises should be encouraged after the onset of facial nerve paralysis. The best outcome of rehabilitation is with biofeedback which can be either with mirror feedback or electromyography. Neuromuscular junction re-education is important to prevent mass muscle movement and improve co-ordination [8].
2. Botulinum toxin
Injection into the orbicularis, platysma, mentalis, frontalis, and corrugator supercilli combined with physical therapy is effective [6],[8].
3. Surgery
Neurolysis and myectomy have been described, but postoperative complications, need for rehabilitation and recurrence make them less popular [8].
Psychogenic facial movement disorder
Psychogenic movement disorders are characterized by bizarre or unwanted movements of a body part or parts caused by an underlying psychological condition or stress. They are diagnosed as per Fahn and William criteria [9]. The criteria include abrupt onset, inconsistency/incongruency, distractibility, false weakness, false sensory changes, pain, exhaustion, excessive startle, bizarre movements, and concomitant somatizations, among others [9].
Psychogenic facial movement disorder (PFMD) involves the orofacial region. The condition is usually seen in young women. Depression and headache are often present.
Clinically patients have phasic or tonic contractions resembling dystonia. Lip pulling downward is the most common feature. The movements are mostly paroxysmal. Frontalis is often hyperactive contralateral to the orbicularis involvement. There may be associated pain in a few cases. Tremor or jerky movements of other parts like limbs, neck, or trunk can be present in a small proportion of patients [10].
There are spontaneous exacerbations and remissions. Distractions reduce facial movements. Psychotherapy helps [10].
Differentiation from HFS [10]:
- Presence of asynchronous, tonic movements in the ipsilateral lower face or synchronous bilateral lower face. HFS has synchronous movements involving one-half of the face.
- Absent Babinski sign in PFMD
- Normal blink response in PFMD. In HFS, the blink response elicited by supra-orbital nerve stimulation spreads to muscles other than orbicularis oculi.
Diagnosis made easy in 4 easy steps (Figure 7):
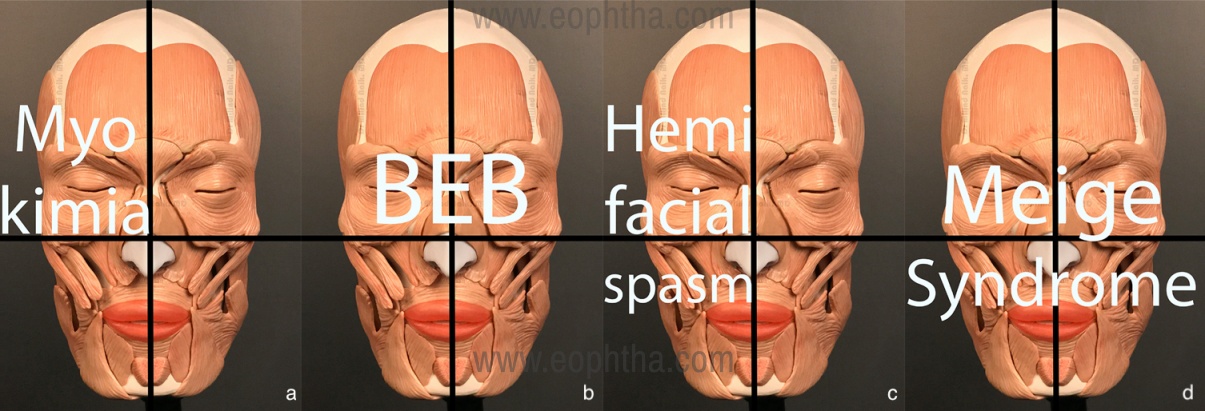
Figure 7: A simple clinical algorithm to identify the basic facial spasms based on the quadrants involved. In myokimia, flickers are noted in only one quadrant ie the eyelids and periocular area (a). The involvement of two quadrants in the upper half of the face is seen in Benign Essential Blepharospasm (b). Involvement of facial muscles in two quadrants on one half of the face divided by the vertical meridian in hemifacial spasm (c). In Meige’s syndrome the spasms are noted in all four quadrants (d).
- Divide the face into 4 quadrants
- Identify the quadrant involved
- Identify the pattern
- Make the diagnosis
|
Orbicularis myokymia |
Benign essential blepharospasm |
Hemifacial spasm |
Meige’s syndrome |
|
|
Area involved |
One quadrant- eye |
2 quadrants- both eyes |
2 quadrants- half of the face |
4 quadrants |
|
Muscles involved |
Orbicularis oculi |
Orbicularis oculi, procerus, corrugator supercilli |
Facial muscles of expression on affected half of face |
Facial muscles of expression, oromandibular muscles- temporalis, masseter; platysma |
|
Age of onset |
5-7th decade |
5-7th decade |
3rd-7th decade |
|
|
Etiology |
Hyperactivity of orbicularis fascicles |
Abnormality in blink reflex |
Vascular compression over facial nerve exit site |
Increased cholinergic and dopaminergic activity |
|
Associations |
Apraxia of eyelid opening in about 4-7% |
|||
|
Investigations |
Not warranted |
Required only in cases of associated neurological manifestations |
Imaging to r/o pathology in region of cerebellopontine / vascular loop compression |
Systemic work-up in cases with clinical suspicion of secondary Meige syndrome. |
|
Treatment |
Stress and sleep management. Reduce caffeine. Stop offending. Drug in case of drug induced myokymia |
-Botulinum toxin injection -Total or subtotal myectomy |
-Vascular decompression neurosurgery -Botulinum toxin injection |
-Oral pharmacotherapy -Botulinum toxin injection -Deep brain stimulation |
Table 2: Comparison of different facial movement disorders
References
- Albanese A, Bhatia K, Bressman SB, et al. Phenomenology and classification of dystonia: a consensus update.Mov Disord. 2013;28:863-873.
- Miller NR. Eyelid myokymia. Surv Ophthalmol. 2011 May-Jun;56:277-8.
- Khalkhali M. Topiramate-Induced Persistent Eyelid Myokymia.Case Rep Psychiatry. 2016;2016:7901085.
- Ross AH, Elston JS, Marion MH, Malhotra R. Review and update of involuntary facial movement disorders presenting in the ophthalmological setting.Surv Ophthalmol. 2011;56:54-67.
- Titi-Lartey OA, Patel BC. Benign Essential Blepharospasm. In:StatPearls. Treasure Island (FL): StatPearls Publishing; August 10, 2020.
- Macintosh PW. Chapter 32: Blepharospasm and Other Facial Spastic Disorders. In: Fay A, Dolman P, eds. Diseases and Disorders of orbit and Ocular adnexa. Elsevier; 2017:1280-1305
- Jahngir MU, Ameer MA, Patel BC. Meige Syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan.Available from: https://www.ncbi.nlm.nih.gov/books/NBK513358/
- Pourmomeny AA, Asadi S. Management of synkinesis and asymmetry in facial nerve palsy: a review article.Iran J Otorhinolaryngol. 2014;26:251-256.
- Shill H, Gerber P. Evaluation of clinical diagnostic criteria for psychogenic movement disorders.Mov Disord. 2006;21:1163-1168.
- Fasano A, Valadas A, Bhatia KP, et al. Psychogenic facial movement disorders: clinical features and associated conditions.Mov Disord. 2012;27:1544-1551.