-21.jpg)

Microbial keratitis is a common vision-threatening disease that occurs in all parts of the world and is an important cause of avoidable corneal blindness. Medical therapy is considered a mainstay in the management of microbial keratitis, however, cases that worsen despite medical therapy or have perforation require surgical management1. Therapeutic keratoplasty is a surgical procedure whose primary purpose is to get rid of the infectious or non-infectious inflammatory tissue along with the restoration of the structural integrity of the eye (tectonic support)2. The surgical procedure, postoperative course, and chances of graft survival in therapeutic keratoplasty are different from optical keratoplasty as surgery is performed on an inflamed eye.
Therapeutic keratoplasty could be
- Therapeutic Penetrating Keratoplasty(ThPK)
- Therapeutic lamellar keratoplasty- Deep Anterior Lamellar Keratoplasty(Th-DALK)
- Patch graft
In therapeutic penetrating keratoplasty, a full-thickness button of the diseased cornea is removed and replaced with a donor corneal graft, whereas in therapeutic lamellar keratoplasty only the diseased cornea is replaced with a partial-thickness donor corneal graft, leaving the posterior cornea (Descemet’s membrane and endothelium) intact. A patch graft is partial or full-thickness graft usually done for tectonic purposes.
Indications for which therapeutic keratoplasty may be required-
Infectious keratitis
- Bacterial
- Fungal
- Viral
- Others- Acanthamoeba, Nocardia, Pythium,etc.
Non-infectious keratitis
- Persistent epithelial defect and sterile melt
- Peripheral ulcerative keratitis(PUK)
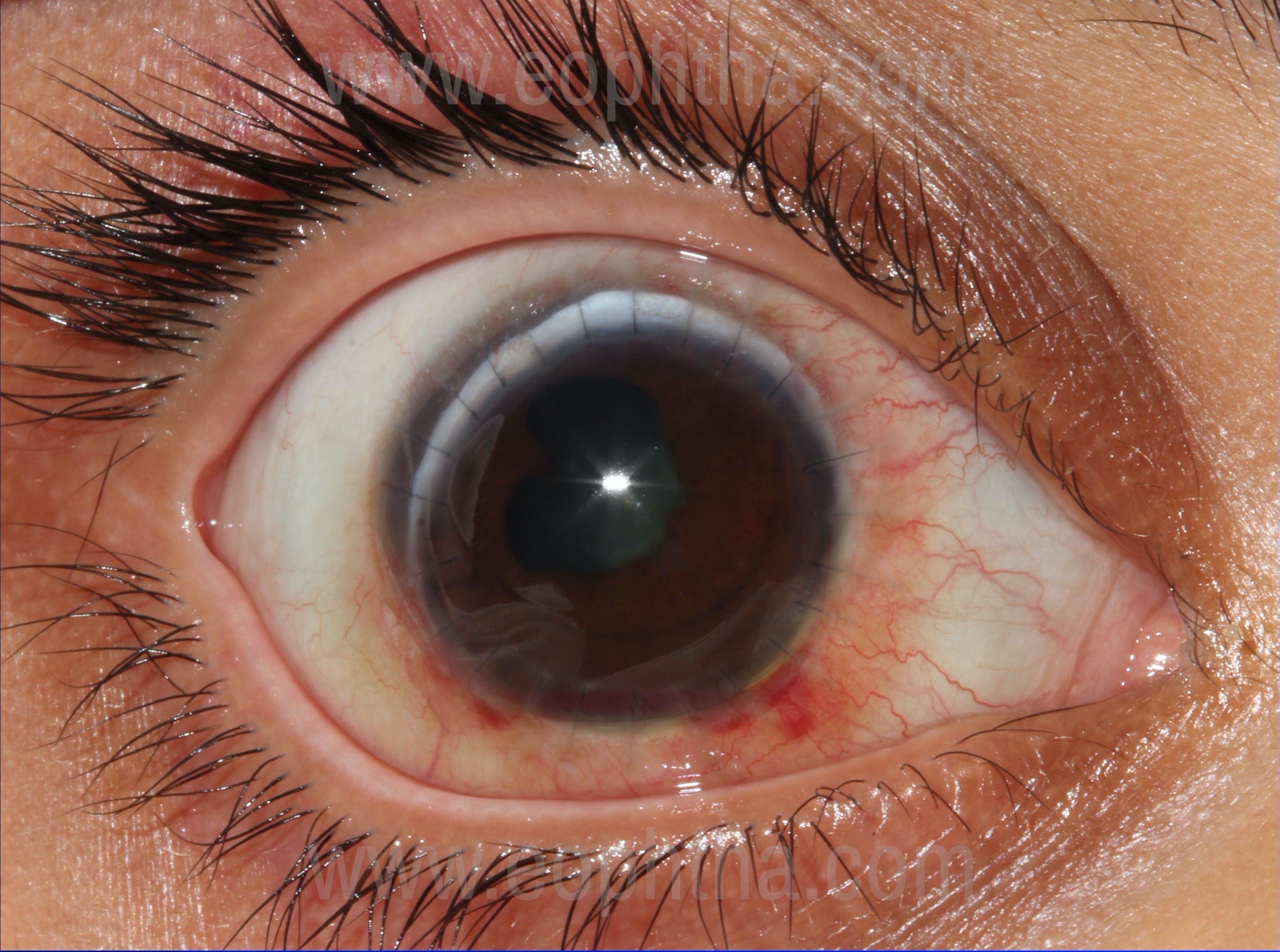
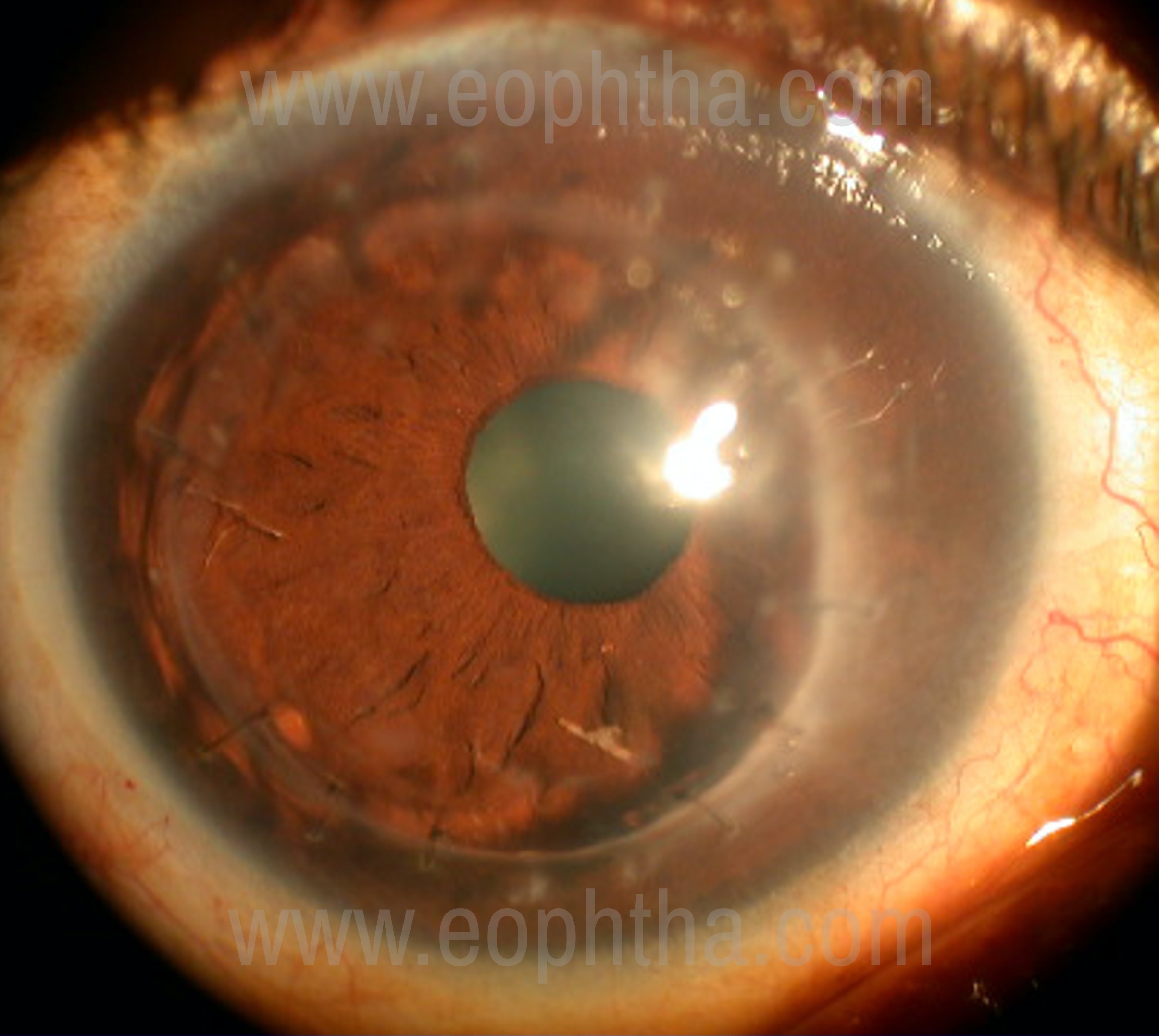
Therapeutic keratoplasty for infectious keratitis:
Microbial keratitis is the most common indication for therapeutic keratoplasty3-4. Even with a better understanding of the pathology of corneal disease and continuing advances in medical management, there remain cases that do not respond to maximal medical therapy5-15. Also, the facilities for basic investigations and appropriate medical management for infectious keratitis are often lacking at the primary and secondary health care centers16. A significant proportion of patients with microbial keratitis progress and often require an emergency therapeutic keratoplasty.
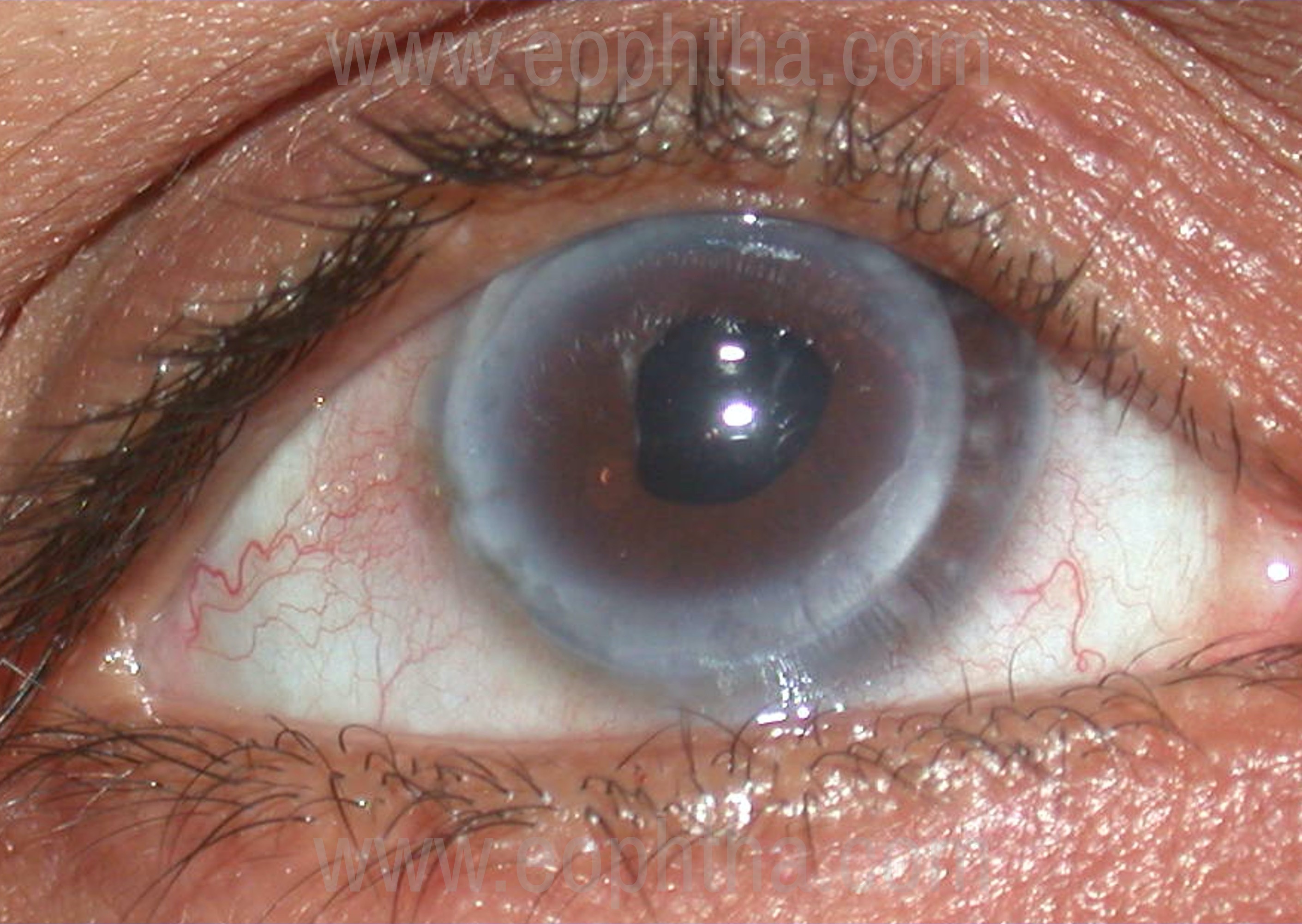
Indications of Surgery
- Refractory/worsening despite optimal medical therapy,
- Progression with risk for limbal/scleral extension,
- Progression to endophthalmitis
- Impending or a frank large perforation.
It provides surgical debridement of an infectious process with a goal to remove the infectious inoculum completely or to decrease the organisms in the cornea to a level at which exogenous anti-microbial agents and the patient's endogenous host defense mechanisms can be effective.
Causative organisms:
In a study from North India by Sharma et.al17 and South India by Gopinathan et.al18,the following are the organisms isolated of all culture-positive infections.
|
Bacterial |
Fungal |
Mixed (Bacterial and Fungal) |
Acanthamoeba |
Viral DNA on PCR |
|
|
North India |
31.0% (Most common Coagulase-negative Staphylococcus 38.8%) |
20.9% (Most common Aspergillus species 39.6%) |
6.9% |
1.6% |
5.3% |
|
South India |
51.9% (Most common Staphylococcus epidermidis 42.3%) |
38.2% (Most common Fusarium 36.6%) |
7.5% |
2.4% |
- |
A significantly larger number of patients (50.8%) with fungal keratitis required surgical intervention compared to bacterial (43.2%) andAcanthamoeba(17.4%) keratitis reflecting the poorer response of fungi and acanthamoeba to medical therapy in general.In a study by Sharma et.al17, the anatomical success of therapeutic keratoplasties with the restoration of tectonic integrity was seen in 89.7%. A higher success rate with isolated bacterial (93.6%) or fungal (88.6%) ulcers were achieved when compared with mixed bacterial and fungal infections (71.4%).
Viral Keratitis:
Herpes simplex keratitis
Therapeutic keratoplasty for herpes simplex keratitis is indicated in two situations19
- Severe stromal keratitis refractory to medical therapy or progressing to perforation and
- Large corneal perforations secondary to persistent epithelial defects with little or no active stromal inflammation (HSV-PEDs).
Herpes zoster keratitis
Neurotrophic corneas in herpes zoster tend to be more severe than herpes simplex keratitis because of which therapeutic keratoplasty in herpes zoster keratitis usually have a worse prognosis than in herpes simplex keratitis. One of the most important prognostic variables for herpes zoster therapeutic keratoplasty is the level of corneal sensation. Therapeutic keratoplasty in patients with herpes zoster keratitis perforations often requires adjunctive therapy, such as conjunctival flaps or tarsorrhaphies. Careful management of the external and corneal disease can improve the outcomes in therapeutic keratoplasty for zoster keratitis20.
With Oral Acyclovir we can achieve close to optical results.
Therapeutic keratoplasty for Non-infectious keratitis:
Therapeutic keratoplasty may be required in non-infectious keratitis due to persistent epithelial defect resulting in the progressive stromal loss. A non-responding persistent epithelial defect progressing to stromal melt and perforation can occur in neurotrophic keratitis, exposure keratitis and severe dry eye of various etiologies21-23. Keratoplasty performed for tectonic purpose in such patients with either impending or actual perforation is termed as ‘tectonic keratoplasty’.
Non-inflammatory peripheral disorders of cornea like Pellucid marginal degeneration and Terrien’s degeneration and inflammatory peripheral disorders like peripheral ulcerative keratitis may sometimes perforate and need therapeutic keratoplasty in the form of a cresentric patch grafts.
Attention must be paid to treat the underlying ocular surface and systemic disease when a therapeutic keratoplasty is advocated in such conditions.
Pre-operative evaluation:
A systematic approach is required to improve success in the treatment of infectious keratitis. A good history and clinical examination are vital to know the nature of infection and plan the treatment. Microbiological evaluation helps to confirm the nature of infection and guides antimicrobial therapy.
History:
A detailed history helps to know the course of disease process, cause of the ulcer and response to the treatment taken. A careful history of the development of disease may point to the existence of underlying predisposing systemic conditions that may influence the course of disease. A full list of drugs used should be obtained to ensure that drugs that have not helped in the past are not repeated.
General Medical Evaluation:
The general medical evaluation must be done prior to surgery as some patients with large perforation, expulsion or young age may require general anesthesia. Control of systemic conditions like diabetes mellitus is mandatory.
Ocular Examination:
A detailed examination prior to surgery is mandatory for proper planning and execution of surgery. A thorough slit lamp examination is required to determine the size and depth of the infiltrate and its relation to the limbus. AC depth should be assessed; cases with flat AC or the presence of anterior synechiae must receive intravenous mannitol to control IOP and reduce vitreous volume. All attempts should be made to know the status of the fundus. When the retina is not visible and the integrity of the globe is not compromised, B-scan ultrasonography should be attempted. B-scan ultrasonography can also assess the vitreous for the possibility of endophthalmitis and show the presence of choroidal detachment in patients with hypotony.
This evaluation facilitates the planning of surgical details, such as the size of the trephine and its optimal placement in the recipient bed to ensure the excision of the diseased cornea. The degree of thinning and the presence of actual perforation should be noted. Extreme care is required in handling cases with gross thinning and perforation. Tissue adhesive could be applied to ensure adequate pressure in eyes with actual perforation before trephination. In eyes with a crystalline lens or posterior chamber intraocular lens, pilocarpine 2% can be given 1 hour prior to surgery in an attempt to constrict the pupil to protect the lens and maintain a posterior lens–iris diaphragm.
Preoperative Treatment:
Antimicrobial therapy should be continued until the cornea is available. Systemic antimicrobial therapy is advocated in deep or perforated keratitis or in scleral extension or suspected endophthalmitis. Steroids have the potential to make infections worse so it is better avoided in infectious keratitis. Patching or temporary glue application may be needed to prevent the prolapse of intraocular structures in perforated eyes.
Donor Material:
Criteria for the selection of donor corneas are similar to optical PKP except in circumstances where waiting for good quality cornea may further complicate the clinical situation. In such circumstances, corneas of sub-optimal quality can be used if all the medical standards are fulfilled24. Similarly, donor cornea qualities are not as important in patch grafts that are of small size and are off the visual axis. Excellent grade corneal tissue offers the possibility of optical keratoplasty like outcomes.
Surgical Techniques:
Special attention must be given while performing corneal transplantation for infectious keratitis other than the basic surgical technique of PKP.
Preoperative procedures:
Anaesthesia:
- General anesthesia: Most of the therapeutic keratoplasties especially with large perforations, apprehensive patients and pediatric patients should be ideally performed under general anesthesia because the peribulbar anesthetic injection can cause expulsion of intraocular contents.
- Local anesthesia: If done under local anesthesia it may be better to give a facial block first by the O’Brien technique and then inject a limited volume of anesthetic to achieve retrobulbar or peribulbar block. This helps to avoid sudden intraocular pressure rise. Peribulbar injection of a mixture of 1% lidocaine with epinephrine and 0.75% bupivacaine mixed with hyaluronidase and sodium bicarbonate produces good akinesia and long anesthesia.
- Intravenous anesthesia for sedation may be helpful before giving a block in anxious and uncooperative patients.
Gentle digital massage to obtain a soft eye may be considered in patients with no risk of perforation.
Adjunctive measures:
Preoperative intravenous mannitol 20%(20 g/100 mL) upto 0.5-1g/kg body weight can be administered half an hour prior to surgery to avoid problems related to positive vitreous pressure. Some surgeons prefer giving oral acetazolamide 250-500mgaround 1-3hours prior to surgery.
Therapeutic Penetrating Keratoplasty Surgical steps:
Exposure
Self-retaining speculum/lid sutures can be used to obtain a good exposure. Care must be taken to avoid external pressure on the globe, particularly in cases with perforation. A Flieringa ring provides good scleral support. Peritomy and hemostasis with wet-field cautery is required in large ulcers reaching upto the limbus which facilitates good clearance of recipient infective rim and proper suturing of the donor graft. A drop of preoperative brimonidine may also reduce intraoperative bleeding.
Preparation of the recipient bed
The goal of surgery is to excise all necrotic or infected tissue during the trephination. Measure the involved area using a caliper. If possible, 1 mm rim of healthy tissue should be removed to leave a stable, non-infected recipient bed. The size of the trephination should be carefully determined by placing the appropriate trephine over the cornea and creating an indentation in the epithelium. Trephination of the recipient bed can be technically difficult, especially in cases with corneal necrosis, gross thinning and actual perforation due to loss of scleral rigidity and low intraocular pressure. Pressure on the globe in such cases can lead to extrusion of intraocular contents and/or expulsive choroidal hemorrhage. It is therefore important to use an extremely sharp trephine and apply minimal pressure. Suction trephines such as Hessburg–Baron trephine can be advantageous under these situations, however aren’t freely available. In eyes with perforation, initial tectonic support can be obtained by applying cyanoacrylate glue during or prior to surgery so that anterior chamber can be re-formed with viscoelastic and host trephination can be done under a controlled environment. A freehand dissection of the recipient after initial marking with trephine may be required in case of large ulcers with large perforation. A limbal stab incision or side port may be useful to sweep iris from the perforation with iris spatula or perform anterior vitrectomy when there is vitreous in the perforation or to fill AC with viscoelastic before trephination to prevent sudden decompression of the globe.
The corneal trephination should be centered over the infection or perforation so as to leave maximal non-infected tissue between the ulceration and recipient bed. In the case of small ulceration or perforation, decentering the graft may give better optical results.
The initial recipient trephination should be up to 80% depth after which a guarded entry should be made into the AC with either no.11 surgical blade or any other sharp blade. Entry should be guarded in shallow AC to prevent injury to the lens in phakic eyes.
The diseased cornea can then be excised completely with right and left Castroviejo scissors. Leaving a relatively wider posterior ledge(nearly 1mm), especially in large grafts, provides support and reduces the risk of postoperative wound leaks.
The recipient corneal button should be divided into two halves. One half should be sent in BSS for microbiology evaluation and the other half in 20%formaldehyde for a histopathology examination. Additionally, exudates in AC, vitreous exudates, iris tissue may need to be submitted to the microbiology laboratory.
Additional procedures:
- Performing minimum intraocular surgery is recommended.
- Anterior chamber irrigation with BSS eliminates all exudative material from AC which helps to prevent the recurrence of infection and reduces complication such as glaucoma.
- Dissection of the membranes over the iris should be done by the irrigating cannula and removed very gently with the forceps to avoid bleeding from the iris surface. Any septic foci on the iris should be excised and sent for microbiology evaluation.
- Two large peripheral iridectomies should be performed to avoid pupillary block postoperatively.
- Intracameral antibiotics/antifungals can be used whenever required.
- The crystalline lens should be left in place, as it provides a barrier against vitreous seeding and infectious endophthalmitis.
- In the case of a significant chamber shallowing with positive vitreous pressure, pars plana vitrectomy can be useful to deepen AC and prevent expulsion of the crystalline lens.
- Vitrectomy should be performed when endophthalmitis is suspected and the vitreous sample is sent for microbiology investigation, followed by intravitreal injection of antimicrobials.
- Cases with anesthetic corneas or significant dry eyes, in which postoperative wound healing may be jeopardized, should either have large tarsorrhaphies or a conjunctival flap at the time of therapeutic keratoplasty. A conjunctival flap is further indicated if the eye has limited visual prognosis. Conjunctival flaps can be used for the treatment of chronic corneal ulcers including perforated and infected ones25.
Preparation of the donor cornea:
Unlike optical keratoplasty donor cornea trephination in therapeutic keratoplasty is performed only after excision of recipient cornea because necrosis of the wound edges may require additional trimming and may alter the size of the graft. It is therefore important to measure the recipient opening horizontally and vertically with a caliper to determine the donor cornea size. In cases of total keratoplasty or sclerokeratoplasty, freehand dissection of the donor cornea is performed. Once the recipient bed size is determined, the trephination of the donor cornea about 0.5mm (recipient button up to 10mm) or 1mm (recipient button more than 10mm) larger than the host trephine should be done.
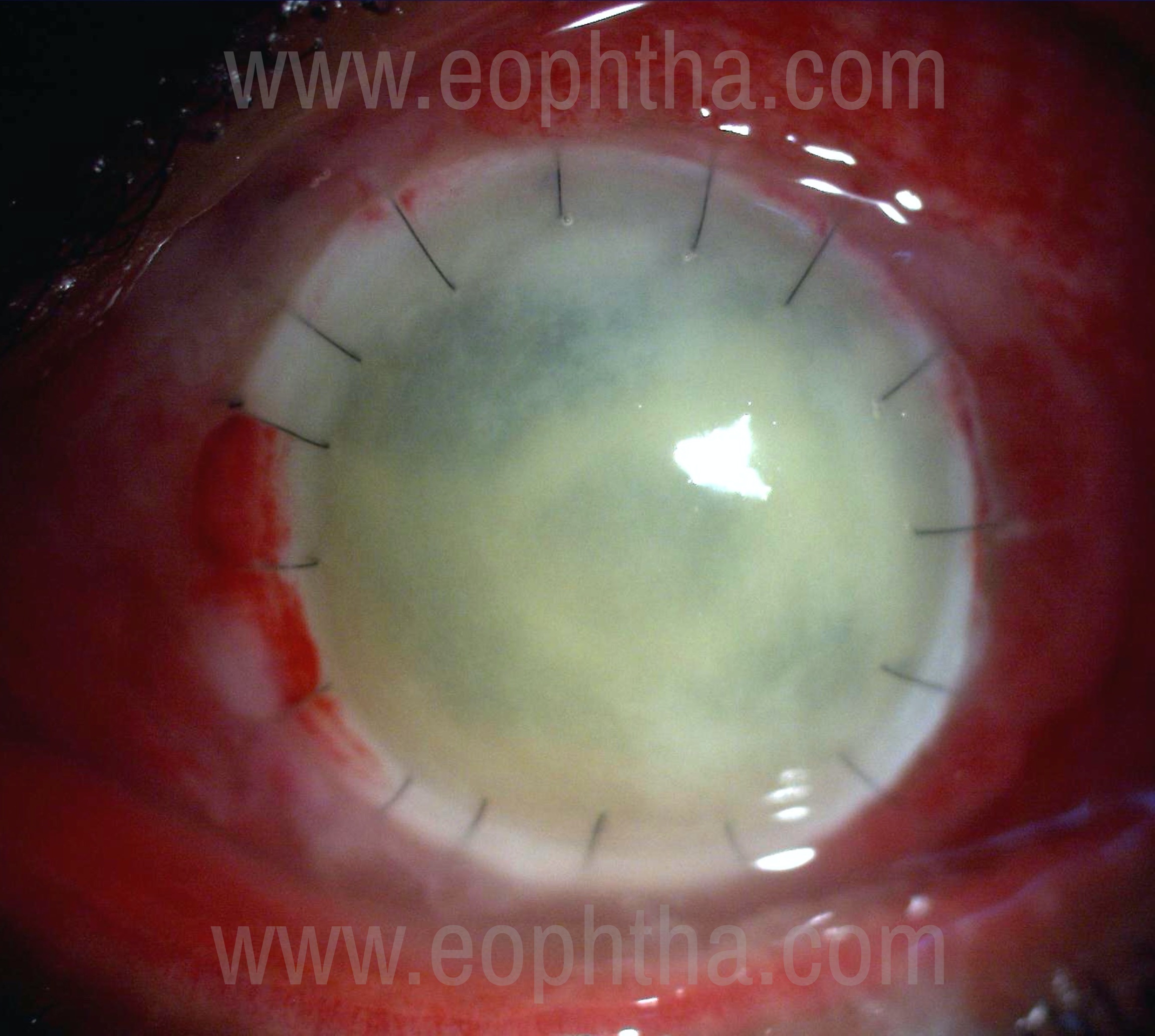
Suturing:
Suturing technique in therapeutic keratoplasty should almost always be interrupted with 10-0 or 9-0 nylon sutures, placed radially and farther into the recipient bed with moderate suture tension to avoid “cheese-wiring” of the sutures through a potentially inflamed host bed. Interrupted sutures allow early suture removal in case of sectoral inflammation, vascularization or recurrent infection. Greater number of sutures (24-32) is often required in therapeutic keratoplasty due to a larger graft size. The integrity of the wound should be ensured at the end of the surgery to prevent the possibility of leakage. Angle supporting sutures may reduce the incidence of postoperative glaucoma.
Therapeutic Lamellar Keratoplasty:
Lamellar therapeutic keratoplasty is done for superficial infections which usually spare deeper stroma and descemets membrane. It can be performed in active microbial keratitis26,27 but it is advisable to avoid in fungal and acanthamoeba keratitis28,29 because of a higher risk of recurrence of infection. It is very important that the lamellar dissection completely removes the infected tissue. Lamellar keratoplasty can also be performed in sterile, non-infective ulcerations30-32.
Surgical Steps:
Preparation of recipient cornea:
All the infected necrotic tissue is removed using a trephine 1mm larger than the size of the lesion. Dissection depth needs to be determined at times by layered dissection, so that all infected tissue is removed and perforation is avoided.
Donor button preparation:
A whole globe or corneo-scleral rim mounted on an artificial chamber is used for donor button preparation however if DALK is done the descemet’s and endothelium is peeled from the button and used in desired size. A donor corneal button of 0.25-0.5mm larger than the recipient is used to avoid wound tension.
Suturing:
The donor graft is secured over the lamellar bed with interrupted 10-0 nylon sutures placed radially.
Advantages of Lamellar over Penetrating Therapeutic Keratoplasty:
- No endothelial rejection.
- Complications due to intraocular procedures are avoided.
- Lower quality donor tissue can be used as healthy endothelium is not required.
Disadvantages of Lamellar over Penetrating Therapeutic Keratoplasty:
- Increased risk of re-infection
- Perforation and need to convert to PKP
- Technically more difficult
- Interface scarring and haze
Patch Graft:
Patch graft may be done for the repair of both peripheral or central descemetoceles and perforations. It is done when a perforation cannot be sealed with tissue adhesive(>2mm) and the area of pathology is small(<4-5mm). It could be lamellar or full-thickness, circular or tailored, scleral or non-optical corneal tissue which could be secured with tissue adhesive33,34.
Modified surgical technique under special circumstances:
Sclerokeratoplasty:
Sclerokeratoplasty involves the transplantation of entire cornea and adjacent scleral rim. It is required for severe infections involving the corneal limbus/sclera. Cobo et.al.proposed the use of sclerocorneal dissection avoiding internal angle structures, coupled with the use of angle-supported mattress sutures to maintain the angle and preserve trabecular meshwork function35.
Differences between Therapeutic and Optical penetrating keratoplasty:
|
Optical PK |
Therapeutic PK |
|
|
Indication |
Corneal scar, keratoconus, PMD (For visual rehabilitation) |
Infection, thinning, perforation (For tectonic support) |
|
Graft size |
About 7.5-8.0mm |
Upto 12mm or as much as to involve the infected area |
|
Sutures |
10’0 Smaller and less tighter |
9’0 or 10’0 Larger and more tighter |
|
Centration |
Important |
Tailored fit/Often eccentric |
|
Peripheral iridectomy |
May or may not be required |
Must/Multiple |
|
Donor tissue |
With good endothelial count |
Good tissue (If available) |
|
Cataractous lens |
Removed |
Preserved unless ruptured |
|
Graft failure |
Less likely |
More likely |
|
Infection recurrence |
Not applicable |
Possible |
|
Visual results |
Good |
Poor |
Postoperative Management:
The postoperative management is as challenging as the surgery itself. Following issues should be dealt with some basic principles:
- Prevent recurrence of infection: Appropriate anti-microbial therapy should be continued postoperatively in case of surgery done for infective keratitis. If the pre-operative diagnosis is not made then histopathology and microbiology evaluation of the excised button is helpful in deciding the postoperative therapy. Organisms like fungus and acanthamoeba need prolonged postoperative anti-microbial therapy.
- Promote re-epithelialization and wound healing: Overtreatment with topical toxic medications should be avoided. Non-preserved tear substitutes, temporary tarsorraphy, and punctal plugs can help in managing difficult situations.
- Use of corticosteroids to control inflammation: The use of corticosteroids following therapeutic keratoplasty for infectious keratitis is controversial. It can be started after 3-7 days of surgery in bacterial or herpetic infections. In fungal and acanthamoeba infections it’s safer to wait for 2-4 weeks depending upon the clinical situation. Corticosteroids should be started with extreme caution after being sure about the complete eradication of the infection.
- Role of Cyclosporine/Tacrolimus: Topical cyclosporine can be used to prevent graft rejection and can avoid the ocular complications like steroid-induced glaucoma. Long term Systemic Immunosuppression with oral cyclosporine has been used in very large grafts in one-eyed individuals or in precious eyes which improves graft survival and vision recovery.
- Intraocular pressure: Raised IOP post-therapeutic keratoplasty may be due to inflammation, angle damage or formation of PAS. The pupil should be dilated to avoid pupillary block post-surgery. Prevention of any glaucomatous damage post-surgery demands aggressive medical and surgical management.
Complications of therapeutic keratoplasty:
Intraoperative complications
- Corneal perforation and expulsion of intraocular contents can occur during local anesthesia
- Retrobulbar hemorrhage, Globe perforation, and Optic nerve injury can occur at the time of local anesthesia
- Iris trauma in the form of iridodialysis, holes in the iris or iatrogenic aniridia can occur due to incomplete, eccentric, or over-aggressive trephination, which is more common in thin or perforated corneas.
- Bleeding can be controlled with viscoelastic, fine-tipped underwater diathermy, topical application of 1:10000epinephrine, or 1:100thrombin on a soaked cellulose sponge and preoperative brimonidine drop.
- Autoexpulsion of intraocular contents in perforated corneas can occur in case of positive vitreous pressure or with aggressive trephination. Positive vitreous pressure can be reduced by mechanical, medical, and surgical methods36-38. Pre-operative assessment and administration of injection mannitol, constriction of the pupil with pilocarpine, mechanical pressure on the globe manually or with a Honan balloon or with a super-pinky(to be avoided in case of perforation), intra-operatively lifting or repositioning the speculum or providing anterior traction on the globe with the fixating suture or pars plana vitrectomy may help to avoid such inadvertent complication.
- Supra-choroidal hemorrhage or expulsive hemorrhage can occur if vitreous up-thrust is thereafter removing the recipient's cornea.
Post-operative complications
- Wound leak and shallow AC- Prompt re-suturing should be attempted.
- Suture problems- Suture infiltrates should be carefully distinguished as infective(solitary, on graft or host side with epithelial defect and/or AC reaction) or inflammatory(multiple, usually on host side with no epithelial defect or AC reaction) so as to manage them accordingly with appropriate anti-microbials or corticosteroids respectively.
- Epithelial defects
-
Causes:
- Unhealthy donor epithelium
- Tear film problems
- Lid and ocular surface problems
- Stem cell loss
- Toxic medications
- Exposure
-
Post-operative treatment:
- Preservative-free lubricant drops and/or ointments
- Epitheliotoxic medication should be avoided/replaced
- Pressure patching can be done for 24-48hours
- Sutures with exposed ends should be removed/replaced
- A soft bandage contact lens can be placed
- Tarsorrhaphy can be performed in non-healing defects
- In case of melts, a conjunctival flap may be useful
- Antivirals- Persistent non-healing defects may also be due to herpes infections
4.Shallow/flat AC–
Causes:
- Wound leak
- Choroidal detachment
- Pupillary block
- Inability to reform at the end of surgery
It needs prompt attention and early reformation.
- Hyphema.
- Raised IOP- Control of post-operative raised IOP is vital as elevated pressure may result in endothelial cell damage38. Causes of elevated IOP in the early postoperative period include retained viscoelastic, intraocular inflammation, trabeculitis, anterior synechiae causing angle closure and pupillary block.
- Inflammation-
- Severe preoperative Inflammation
- Excessive surgical manipulation
- Inability to use steroids early on
- Recurrence of Primary Infection in the Graft-
Recurrence of Primary Infection in the Graft
Causes:
- Incomplete excision of infected tissue
- Residual infected iris or anterior chamber exudates
- Associated vitreous involvement/Endophthalmitis
- Early administration of steroids
- Resistance to antimicrobials
Management:
- Medical therapy based on culture sensitivity
- AC wash/Intracamerals
- Absolute Alcohol application and cryotherapy(Pythium)
- Regraft of a larger size
- Endophthalmitis– Incidence is 0.1%-2%38,The prognosis for endophthalmitis after corneal transplantation has been very poor39. Infections in immediate post-keratoplasty period are mostly due to recurrence of host infection but a contaminated donor button or intraoperative contamination can occur as with any surgery.
- Primary graft failure- Irreversible edema of the corneal graft in the immediate postoperative period due to poor donor tissue or surgical trauma to the donor endothelium.
- Cataract due to inflammation or surgical trauma.
- Glaucoma- Pre-existing glaucoma and AC distortion can lead to the development of post keratoplasty glaucoma. The increased incidence of glaucoma could be due to inflammatory sequelae(iritis, trabeculitis, peripheral anterior synechiae, and posterior synechiae), suturing technique (angle compression, trabecular meshwork collapse, and iridocorneal adhesions) or drug-induced(corticosteroids and viscoelastic substances). Pupillary block, ghost-cell or misdirected aqueous or ciliary block (malignant)glaucoma are some of the other causes of post keratoplasty glaucoma. Inadequate IOP control post keratoplasty is one of the leading causes of graft failure. Initial management to reduce IOP is done with topical or systemic antiglaucoma medications. Despite significant risk to the graft with any procedure, surgical intervention is required when IOP is not controlled with topical or systemic medications. Trabeculectomy with or without antimetabolites, Seton devices, endoscopic cyclophotocoagulation, or trans-scleral Nd: YAG laser cyclophotocoagulation may be required but the rate of graft failure and complications are significant after any of these procedures.
- Secondary Graft failure-
-
- Graft rejection
- Chronic Inflammation
- Endothelial decompensation
- Recurrence of infection.
for Fungal keratitis
- Phthisis bulbi- Severe inflammation can cause alteration and disorganization of intraocular structures and atrophy.
References:
- Ang M, Mehta JS, Arundhati A, Tan DT (2009) Anterior lamellar keratoplasty over penetrating keratoplasty for optical, therapeutic, and tectonic indications: a case series. Am J Ophthalmol 147 (4):697–702 e692. doi:10.1016/j.ajo. 2008.10.002
- Yalniz-Akkaya Z, Burcu A, Doğan E, et al. Therapeutic penetrating keratoplasty for infectious and non-infectious corneal ulcers. Int Ophthalmol. 2015;35(2):193–200.
- Tragakis MP, Rosen J, Brown SI. Transplantation of the perforated cornea. Am J Ophthalmol 1974;78:518-22
- Arentsen JJ, Laibson PR, Cohen EJ. Management of corneal descemetoceles and perforations. Ophthalmic Surg 1985; 16: with antimicrobial drugs in the treatment of infectious cor29-33.
- Ti SE, Scott JA, Janardhanan P, et al. Therapeutic keratoplasty for advanced suppurative keratitis. Am J Ophthalmol. 2007; 143(5):755–762.
- Hill JC. Use of penetrating keratoplasty in acute bacterial keratitis. Br J Ophthalmol. 1986;70:502–506.
- Forster RK, Rebell G. Therapeutic surgery in failures of medical treatment for fungal keratitis. Br J Ophthalmol. 1975; 59:366–371.
- Hill JC. Use of penetrating keratoplasty in acute bacterial keratitis. Br J Ophthalmol 1986; 70: 502–506.
- Ross J, Roy SL, Mathers WD, et al. Clinical characteristics of Acanthamoeba keratitis infections in 28 states, 2008 to 2011. Cornea. 2014;33(2):161–168.
- Panda A, Khokhar S, Rao V, et al. Therapeutic penetrating keratoplasty in non-healing corneal ulcer. Ophthalmic Surg 1995; 26: 325–329.
- Chen WL, Wu CY, Hu FR, et al. Therapeutic penetrating keratoplasty for microbial keratitis in Taiwan from 1987 to 2001. Am J Ophthalmol 2004; 137: 736–743.
- Polack FM, Kaufman HE, Newmark G. Keratomycosis: medical and surgical management. Arch Ophthalmol 1971; 85: 410–416.
- Xie L, Dong X, Shi W. Treatment of fungal keratitis by penetrating keratoplasty. Br J Ophthalmol 2001; 85: 1070–1074.
- Tanure MA, Cohen EJ, Sudesh S, et al. Spectrum of fungal keratitis at Wills Eye Hospital, Philadelphia, Pennsylvania. Cornea 2000; 19: 307–312.
- Garg P, Gopinathan U, Choudhary K, et al. Keratomycosis: clinical and microbiologic experience with dematiaceous fungi. Ophthalmology 2000; 107: 574–580.
- Lim AS. Mass blindness has shifted from infection (onchocerciasis, trachoma, corneal ulcers) to cataract. Ophthalmologica. 1997;211:270.
- Sharma N, Jain M, Sehra SV, et al. Outcomes of therapeutic penetrating keratoplasty from a tertiary eye care centre in northern India. Cornea. 2014;33(2):114–118
- Gopinathan U, Sharma S, Garg P, et al. Review of epidemiological features, microbiological diagnosis and treatment outcome of microbial keratitis: experience of over a decade. Indian J Ophthalmol. 2009;57: 273–279.
- Killingsworth DW, Stern GA, Driebe WT, et al. Results of therapeutic penetrating keratoplasty Ophthalmology. 1993;100:534–541
- Tanure MA, Cohen EJ, Grewal S, et al. Penetrating keratoplasty for varicella-zoster virus keratopathy. Cornea. 2000;19:135–139
- Palay DA, Stulting RD, Waring GO III, et al. Penetrating keratoplasty in patients with rheumatoid arthritis. Ophthalmology 1992; 99: 622–627.
- Bernauer W, Ficker LA, Watson PG, et al. The management of corneal perforations associated with rheumatoid arthritis. An analysis of 32 eyes. Ophthalmology 1995; 102: 1325–1337.
- Vanathi M, Sharma N, Titiyal JS, et al. Tectonic grafts for corneal thinning and perforations. Cornea 2002; 21: 792–797.
- Yao YF, Zhang YM, Zhou P, et al. Therapeutic penetrating keratoplasty in severe fungal keratitis using cryopreserved donor corneas. Br J Ophthalmol 2003; 87: 543–547
- Khodadoust A, Quinter AP. Microsurgical approach to the conjunctival flap. Arch Ophthalmol. 2003;121(8):1189–1193.
- Xie L, Shi W, Liu Z, et al. Lamellar keratoplasty for the treatment of fungal keratitis. Cornea 2002; 21: 33–37.
- Tong L, Tan DT, Abano JM, et al. Deep anterior lamellar keratoplasty in a patient with descemetocele following gonococcal keratitis. Am J Ophthalmol 2004; 138: 506–507.
- Vemuganti GK, Garg P, Gopinathan U, et al. Evaluation of agent and host factors in progression of mycotic keratitis: a histologic and microbiologic study of 167 corneal buttons. Ophthalmology 2002; 109: 1538–1546.
- Anderson B, Roberts SSJ, Gonzales C, et al. Mycotic ulcerative keratitis. Arch Ophthalmol 1959;62:169–79.
- Bessant DA, Dart JK. Lamellar keratoplasty in the management of inflammatory corneal ulceration and perforation. Eye 1994; 8: 22– 28.
- Soong HK, Farjo AA, Katz D, et al. Lamellar corneal patch grafts in the management of corneal melting. Cornea 2000; 19: 126–134.
- Titiyal JS, Ray M, Sharma N, et al. Intralamellar autopatch with lamellar keratoplasty for paracentral corneal perforations. Cornea 2002; 21: 615–618
- Sharma A, Mohan K, Sharma R, et al. Scleral patch graft augmented cyanoacrylate tissue adhesive for treatment of moderate-sized noninfectious corneal perforations (3.5–4.5mm). Cornea. 2013; 32(10):1326–1330.
- Khalifa YM, Bailony MR, Bloomer MM, et al. Management of nontraumatic corneal perforation with tectonic drape patch and cyanoacrylate glue. Cornea.2010; 29(10): 1173–1175.
- Cobo M, Ortiz JR, Safran SG. Sclerokeratoplasty with maintenance of the angle. Am J Ophthalmol 1992; 113: 533–537
- Kirsch RE, Steinman W. Digital pressure, an important safeguard in cataract surgery. Arch Ophthalmol 1955; 54(5): 697–703.
- Kirsch RE. Further studies on the use of digital pressure in cataract surgery. Arch Ophthalmol 1957; 58(5): 641–646.
- Quist LH, Stapleton SS, McPherson SD Jr. Preoperative use of the Honan intraocular pressure reducer. Am J Ophthalmol 1983; 95(4): 536–538.
- Guss RB, Koenig S, Dela Pena W, et al. Endophthalmitis after penetrating keratoplasty. Am J Ophthalmol 1983; 95: 651–658