
Development of the lacrimal secretory apparatus:
The lacrimal gland develops from solid ectodermal buds in the anterior superolateral part of the orbit. The gland does not start functioning fully until approximately 6 weeks after birth.
Newborn infants do not produce tears while crying.
Development of the lacrimal excretory system:
The Nasolacrimal duct opens in the inferior meatus of the nose. Failure of the caudal end to canalize at birth results in congenital nasolacrimal duct obstruction, which resolves spontaneously in the majority of cases within 4-6 weeks of birth.
Anatomy of the lacrimal system:
The lacrimal secretory apparatus
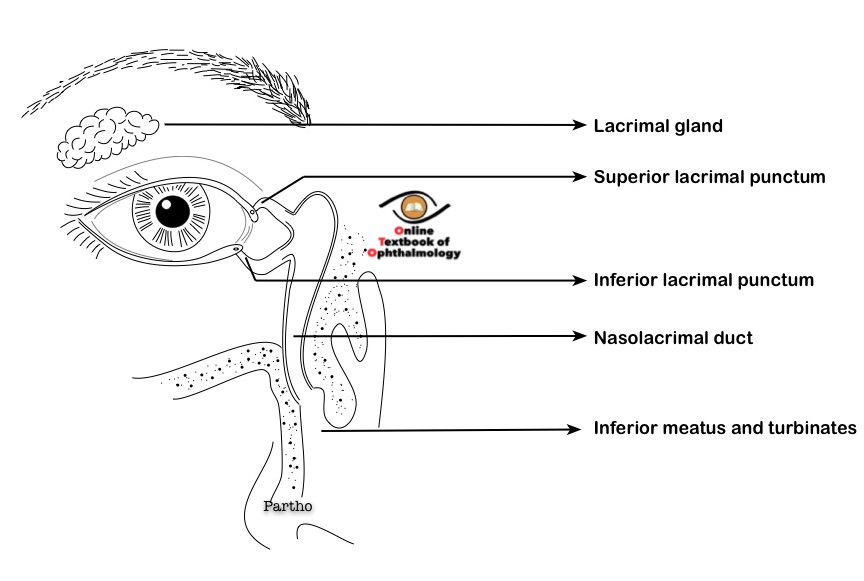
Tears are secreted by the main and accessory lacrimal glands. The main lacrimal gland is located in the lacrimal gland fossa in the superotemporal quadrant of the orbit. The lacrimal gland has two lobes, the larger almond-shaped orbital, and the smaller palpebral lobe. These lobes are divided by the lateral horn of the levator aponeurosis. The palpebral lobe can be seen by everting the upper lid. The ducts from the orbital lobe traverse the palpebral lobe and finally open in the superior conjunctival fornix.
Removal or damage to the palpebral part of the lacrimal gland can reduce tear secretion from the entire gland. Hence lacrimal gland biopsy is done from the orbital lobe.
The accessory lacrimal glands - glands of Krause and Wolfring, are located in the superior conjunctival fornix and the upper tarsal border respectively.
The lacrimal excretory apparatus:
Puncta and canaliculi:
The lacrimal excretory system starts from the lacrimal puncta which lies at the medial ends of both upper and lower lids. Each puncta is surrounded by its respective ampulla and leads into the canaliculi. The canaliculus has a 2 mm long vertical portion and an 8 mm long horizontal portion.
In more than 90% of individuals both the upper and lower canaliculi join to form a common canaliculus which then enters into the lacrimal sac.
The Lacrimal sac:
A membranous valve of Rosenmuller lies at the junction of the common canaliculus and lacrimal sac. This valve prevents the reflux of tears into the canalicular system. The lacrimal sac lies in the lacrimal sac fossa which is bound by the anterior and posterior lacrimal crests. The length of the lacrimal sac is around 12-15 mm. The anterior and posterior crus of the medial canthal tendon encircle the fundus of the lacrimal sac and attaches to the anterior and posterior lacrimal crests respectively. The deep head of preseptal Orbicularis oculi (Horner’s muscle) helps in pumping the tears accumulated in the lacrimal sac.
The superior portion of the lacrimal sac is lined with fibrous tissue. This may explain why lacrimal sac distention does not extend superiorly beyond medial canthal tendon
Nasolacrimal duct (NLD):
The lacrimal sac continues inferiorly into the nasolacrimal duct. The NLD is 12-18 mm in length and travels within the bony nasolacrimal canal in a downward backward and lateral direction. The duct finally opens into the inferior meatus of the nose. This opening into an inferior meatus is partially covered by a mucosal fold, the valve of Hasner.
The tear reflex:
The tear reflex is a complex pathway. The afferent innervation of this pathway is served by the ophthalmic branch of the trigeminal nerve. The efferent pathway is provided by the parasympathetic fibers through the greater superficial petrosal branch of facial nerve via the sphenopalatine ganglion.
Physiology:
The Tear Film:
The average thickness of tear film is around 7-8 µm and the average volume is around 7 µl. The tear film is composed of three layers, the outer lipid layer, the middle aqueous layer, and the innermost mucin layer.
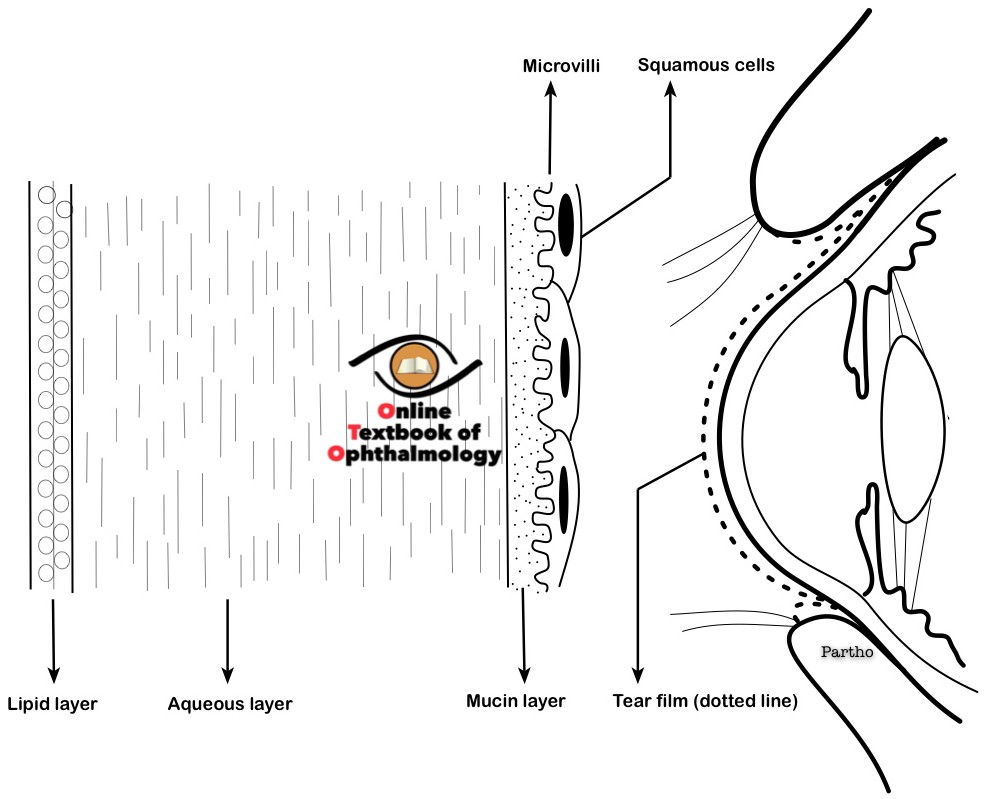
Lipid layer:It is the anterior-most portion of the tear film and is composed of lipids secreted by the meibomian glands. Meibomian glands are modified sebaceous glands present in the tarsal plate of the upper and lower lids. The sebaceous glands of Zeis are located at the eyelid margin close to the roots of eyelashes. The glands of Zeis also secrete lipids which get incorporated into the tear film. The lipid layer has the following functions:
- Decreases evaporation of the tear film
- It helps in maintaining the optical properties of the tear film
- Prevents tear overflow by maintaining a hydrophobic barrier
- Prevents damage to lid margin skin
Aqueous Layer:the aqueous layer constitutes the middle layer of the tear film. It is secreted by the main and accessory lacrimal glands. The aqueous layer constitutes more than 90% of the tear film. This layer consists of electrolytes, water, proteins and a variety of other solutes. It also contains antibacterial substances like lysozyme, betalysin, and lactoferrin The aqueous layer has the following functions:
- Constitutes the major portion of the tear film
- Provides nutrients and oxygen to the cornea
- Prevents infection due to its antibacterial properties
Mucin layer:The mucin layer is secreted by the conjunctival goblet cells. It forms the innermost layer of the tear film. The mucin layer converts the hydrophobic corneal surface into a hydrophilic one.
Physiology of tear drainage:
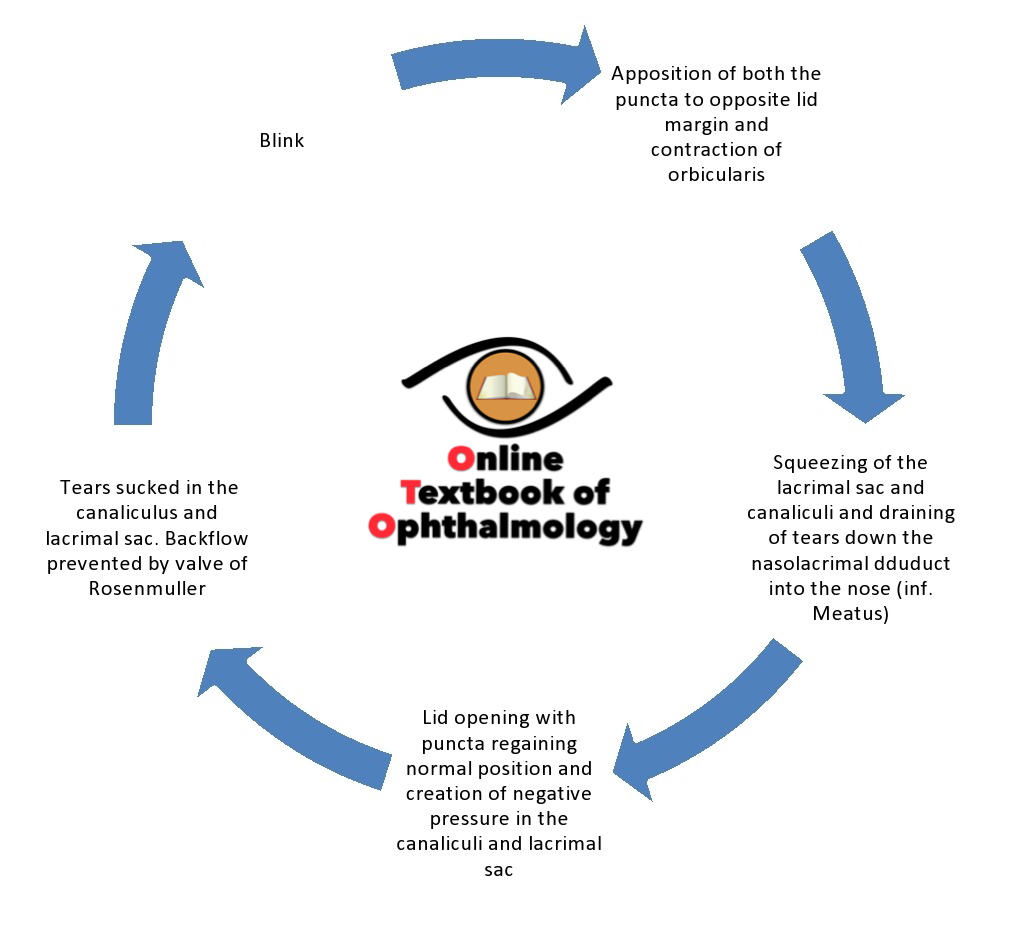
Approximately 10-20% of tear drainage is carried out by evaporation. Most of the tear flow from the eye to nose through the nasolacrimal system is by an active pump mechanism of orbicularis oculi. With each blink the orbicularis contracts and thus squeezes the lacrimal sac, forcing out the tears collected before the blink, down the nasolacrimal duct. During the blink both the puncta remain apposed to the lid margin thus preventing any backward regurgitation of tears. As the eye opens up after the blink both the puncta open up and the tear gets sucked in the lacrimal sac by the negative pressure. The same cycle continues on with each blink.
Evaluation of the watering eye:
Watering of the eye may occur either due to excessive secretion of tears (hyperlacrimation) or a decrease in tear drainage (epiphora).
|
Hyperlacrimation |
Epiphora |
|
1. Primary hyperlacrimation:Rare and occurs due to direct stimulation of the lacrimal gland either due to a lacrimal gland pathology or under the effect of parasympathetic drugs. |
1. Physiological:It results from lacrimal pump failure. ( Orbicularis occuli weakness, seventh nerve palsy, eyelid laxity) |
Evaluation of the lacrimal excretory system:
Clinical history and examination:Detailed history should be taken regarding the duration and severity of watering. Negative history to rule out all possible causes as detailed above should be taken. Any past history of lacrimal surgery should be asked. Examination starts from the diffuse light examination which includes looking at the tear meniscus height, position of the lids and puncta, swelling in the lacrimal sac region, and any lid or ocular surface pathology. The scar mark in the sac area should also be carefully examined. The lacrimal sac area is swollen, erythematous and tender in cases of acute dacryocystitis. A fluctuant tender swelling in the sac area signifies a sac abscess. A non-tender swelling in the lacrimal sac area is seen in cases of lacrimal sac mucocoele or neoplasm.
Some special tests are done to further evaluate the cause of epiphora. These are as follows and are routinely done in any case presenting with epiphora.
Regurgitation test:A steady pressure with the thumb is applied over the lacrimal sac area below the medial palpebral ligament.Regurgitation of fluidOnPressure over theLacrimalSac (ROPLAS) is indicative of an obstruction in the lower lacrimal drainage system. The fluid may be clear, mucoid or frankly purulent depending on the quantum of infection present in the lacrimal sac.

Dye disappearance test:The fluorescein dye disappearance test (DDT) is done to evaluate for lacrimal drainage failure. Fluorescein dye is instilled into the inferior fornix and evaluated under the slit lamp for residual dye present 2 minutes after installation. Normally there should not be any dye present in the conjunctival cul de sac. Retention of dye indicates inadequate drainage whereas the absence of dye in a patient presenting with watering signifies hyperlacrimation. It is a useful test to assess the lacrimal drainage system in children.
Lacrimal syringing :It is performed after instilling 0.5% paracaine. Normal saline is instilled into the lacrimal sac through punctum with help of syringe and canula.

Following are the possible results obtained after the lacrimal syringing test :
- Free passage of saline from lacrimal passage into nose → no anatomical obstruction.
- Fluid regurgitating through the same punctum → canalicular block
- Immediate clear fluid regurgitating through the opposite punctum with negative ROPLAS → common canalicular block
- Delayed regurgitation of fluid (clear, mucoid or purulent) from the opposite punctum with positive ROPLAS → nasolacrimal duct block
Probing: Probing is performed when a canalicular block is suspected during syringing. It is done to determine the site of the block in the canaliculus. After anesthetizing the conjunctival sac with topical proparacaine 0.5% and dilating the punctum the lacrimal probe is passed into the canaliculus initially vertically for 2mm and then horizontally till it is stopped by the obstruction.
If the block is within 6mm of the punctum then it is a proximal canalicular obstruction; an obstruction beyond 6 mm is a distal canalicular block.
Jones dye tests:Jones dye test is performed when partial obstruction of the lacrimal pathway is suspected. It has got no role in complete obstruction. The test involves instilling 2% fluorescein dye in the conjunctival cul de sac and placing a cotton bud in the inferior meatus of the nose. Recovery of the dye in the inferior meatus after 5 minutes will stain the cotton bud and the test is considered positive. An unstained cotton bud signifies the inability of reaching the dye in the nose and hence negative. The test is performed in two steps and is known as primary Jones or Jones 1 and secondary Jones or Jones 2 respectively.
Primary Jones test or Jones 1: To differentiate between hypersecretion and partial obstruction
Secondary Jones test or Jones 2: To differentiate between partial obstruction and lacrimal pump failure.
Investigations:
Contrast dacrocystography :
Indications:
- Suspected lacrimal sac mass
- Dacryolith
- Traumatic nasolacrimal duct obstruction
Conventional dacryocystography (DCG) is performed by injecting a radiographic contrast material (lipiodol) into the lacrimal drainage passageway with a canula. X rays are taken after 5 minutes and 30 minutes. DCG is done to confirm the site of nasolacrimal dust obstruction to diagnose diverticulae, fistulae and filling defects caused by stones or tumors.
Nowadays DCG is performed after instilling radiopaque dye in drop forms which avoid the use of a canula. CT scan can be done instead of X-ray (CT-DCG) which gives a more clear idea of the surrounding bony structures. (Figure 9)
Nuclear lacrimal scintigraphy :
It is a non-invasive technique that assesses tear drainage under physiologic conditions. A radioactive tracer technetium 99 is instilled in the conjunctival sac and its passage through the lacrimal drainage system is visualized with a gamma camera. This test is useful in assessing incomplete block and obstruction beyond lacrimal sac
Disorders of the lacrimal system:
Developmental disorders of the lacrimal system
Developmental disorders of the lacrimal secretory system
Congenital abnormalities of the lacrimal glands are relatively rare and include hypoplasia or agenesis of the lacrimal gland. Occasionally children are born with ectopic lacrimal glands and lacrimal gland fistula.
Developmental disorders of the lacrimal excretory system
Developmental abnormalities of the lacrimal excretory system include duplication of puncta, punctual aplasia, and hypoplasia, congenital lacrimal cutaneous fistula, congenital nasolacrimal duct obstruction, mucocele, and amniontocele. Congenital nasolacrimal duct obstruction is the most common developmental abnormality of the lacrimal excretory system.
Congenital nasolacrimal duct obstruction (CNLDO):
It usually caused by a membranous block at the level of the valve of Hasner covering the nasal end of the nasolacrimal duct. It may be present in about 50% of newborn infants. However, it is clinically evident in 2-6% of patients as rate of spontaneous resolution is very high. (90% in the first year of life).
Signs and symptoms:
The main complaint is persistent watering from the eyes which usually starts a few weeks after birth. The symptoms get aggravated with cold and cough. Occasionally the child may present with chronic conjunctivitis or acute dacryocystitis.
The common signs are:
- Raised tear film height
- Matting of eyelashes
- Prolonged fluorescein dye disappearance test
- Positive ROPLAS
Management:Approximately 90 % of all symptomatic congenital NLD obstructions resolve in the first year of life. The management options available are:
- Lacrimal Sac Massage (Criggler’s Massage):The parents are taught to perform regular lacrimal sac massage till the child attains 1 year of age. The massage opens up the block by the hydrostatic pressure of fluids being pushed down the nasolacrimal duct manually. Topical antibiotics can be prescribed if the discharge is severe, but their long term use should be discouraged.
- Therapeutic probing and syringing:if the CNLDO fails to resolve with lacrimal sac massage even after 1 year of age therapeutic probing of the nasolacrimal duct is carried out. The procedure can be combined with additional procedures like infracture of the inferior turbinate or a silicone tube intubation depending upon the clinical situation. The silicone tube is usually removed after 3-6 months.
- Dacryocystorhinostomy:DCR is a procedure in which the normal lacrimal pathway is bypassed and an alternative drainage pathway is surgically created which opens in the middle meatus. The procedure is generally performed after 2 years of age. It is indicated in cases in which probing has failed or where probing can not be done because of a bony block or extensive developmental abnormalities of the drainage pathway.
Acquired Disorders of the Lacrimal Apparatus:
Disorders of the lacrimal secretory system:
Inflammation of the lacrimal gland:
Inflammation of the lacrimal gland is known as dacryoadenitis. It can either be a manifestation of idiopathic orbital inflammatory disease (IOID) or infective. Both types present with painful enlargement of the lacrimal gland with S-shaped ptosis of the upper lid.
Bilateral lacrimal gland inflammation can be associated with systemic diseases like sarcoidosis.
Infective dacryoadenitis generally results from bacterial and viral infections. Mumps and Epstein Barr virus are commonly implicated.
Neoplasms of the Lacrimal Gland:
Pleomorphic adenoma or mixed lacrimal gland tumor is the most common benign tumor of the lacrimal gland. It presents with a painless mass in the lacrimal gland regions with S-shaped ptosis of the upper lid. CT or MRI of the orbit is needed for determining the extent of the lesion. Complete excision along with the capsule is the treatment of choice. Recurrences are possible if the capsule ruptures during surgery.
Adenoid cystic carcinoma or cylindroma is the most common malignant tumor of the lacrimal gland. The tumor is painful because of perineural invasion and bony destruction. The tumor is highly malignant and prognosis for life is generally poor.
Up to 50% of lymphoproliferative lesions of orbit present in the lacrimal gland.
C. Dry Eye
Dry eye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tears film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface. Various etiological factors have been implicated in the development of the dry eye, the important ones are summarized as follows.
Clinical features:
Symptoms:Symptoms of dry eye include foreign body sensation, irritation, the sensation of dryness, burning, pain, and photophobia.
Signs:Signs of dry eye should be looked for starting from lid margin upto cornea. They include blepharitis and meibomitis, reduced or absent marginal tear strip, conjunctival congestion and xerosis, corneal epitheliopathy and corneal filaments.
Clinical tests to evaluate the Tear Film:
1. Schirmer’s test :
Schirmer’s test is done to quantify the amount of tear secretion. It can be done without instilling any anaesthetic drops (Schirmer’s I) or after instilling topical anesthetics (Schirmer’s II)
Schirmer’s I measure basic and reflex tear secretion. Schirmer’s II measures basic secretion. It is performed using Whatman filter paper (no 41) 5mm wide and 35 mm long. The filter paper is folded 5mm from one end and kept in lower fornix at the junction of lateral one third and medial two-third. The patient is asked to keep the eyes open. After 5 minutes of filter paper is removed and the amount of wetting from the fold is measured. The value of > 15 is considered normal. Values of 5-10 mm signify moderate dry eye whereas < 5 mm indicates a severe dry eye

2.Tear film break up time (TBUT):
It is the time interval between a complete blink and appearance of first dry spot on precorneal tear film. Fluorescein dye is instilled in lower fornix and after complete blink tear film is examined at slit lamp under cobalt blue filter. After an interval black spots appear in fluorescein stained film, indicating formation of dry areas. TBUT is an indicator of mucin component of tears. Its normal value ranges from 15 to 35 seconds and TBUT of < 10 seconds suggests unstable tear film.
Rose Bengal staining:Rose Bengal is a dye having an affinity for dead and devitalized epithelial cells that have lost or altered mucous layers. A 1% solution of Rose Bengal or a moistened impregnated strip can be used. Depending upon severity staining patterns are observed.
Management:
General measures:General measures for the management of dry eye include maintaining good lid hygiene, conscious frequent blinking while working on computers, wraparound and dark glasses while outdoors and reducing room temperature to minimize evaporation of tears.
Topical tear substitutes:Topical lubricants in the form of drops or ointments remain the mainstay of treatment for dry eye. They contain either polyvinyl alcohol, methylcellulose or hypromellose.
Topical steroids:Topical steroids are used to reduce the surface inflammation so that tear substitutes can act properly
Topical cyclosporine:Topical 0.05% and 0.1% cyclosporine are very effective in cases of severe dry eyes. It helps by reducing the cell-mediated inflammation.
Mucolytics: Mucolytics like 5% acetylcysteine is used in cases of corneal filaments and plaques
Punctal occlusion:Punctal occlusion either by punctal plugs or by cauterization helps in decreasing the tear drainage and thereby reducing the severity of dry eyes. It is generally done in cases of severe dry eyes.
Disorders of the lacrimal excretory system:
A.Obstruction of the lacrimal excretory system:
Obstruction of the lacrimal excretory system can be either at the level of Puncta, canaliculi, lacrimal sac, or nasolacrimal duct. Various causes of obstruction in the lacrimal drainage system have already been mentioned in the evaluation of the watering section. Here we will be discussing nasolacrimal duct obstruction (NLDO) in detail.
Nasolacrimal duct obstruction (NLDO):
Nasolacrimal duct obstruction can be either primary (Primary Acquired Nasolacrimal Duct Obstruction, PANDO) or secondary (Secondary Acquired Lacrimal Duct Obstruction, SALDO).
Primary NLDO is more common than secondary. PANDO is more common in female sex because of the comparatively narrower bony canal. It is common in patients of lower socioeconomic status because of poor hygiene. There is otherwise no known causing factor for PANDO.
Causes of SALDO:
- Trauma
- Inflammation of the lacrimal sac (Wegener's granulomatosis, sarcoidosis)
- Nasal pathology: Hypertrophied inferior turbinate, marked DNS, tumors
- Infections of the lacrimal sac: Tuberculosis, Rhinosporodiosis
- Lacrimal sac neoplasms.
Clinical features:
Patients suffering from NLDO most commonly present with the complaints of watering associated with discharge. This watering of eyes (epiphora) should be differentiated from watering resulting from secondary hyperlacrimation as already described. Long-standing NLDO results in chronic dacryocystitis with repeated attacks of superimposed acute infections (acute dacryocystitis).
Positive ROPLAS is a confirmatory sign of NLD obstruction and no further diagnostic tests are required. However, ROPLAS should be avoided in cases of acute dacryocystitis.
Complications:
Complications of acquired NLD obstruction include
- Acute dacryocystitis (Fig. 12) leading to lacrimal sac abscess, conjunctivitis, even orbital cellulitis
- Chronic dacryocystitis
- Lacrimal sac mucocele
- Lacrimal sac fistula
- Ectropion of lower lid due to chronic wiping of tears and loosening of canthal tendons
- Lower lid eczema
- Any intraocular surgery if performed in the presence of NLD obstruction can lead to endophthalmitis
Management:
- Dacryocystorhinostomy (DCR):Dacryocystorhinostomy is the surgical procedure of choice for NLDO. It involves bypassing the normal nasolacrimal tract and creating a pathway between the lacrimal sac and the middle meatus of the nose.
- Dacryocystectomy (DCT):Dacryocystectomy involves excising and removing the whole lacrimal sac. There are no chances of dacryocystitis and mucoid discharge after DCT, but watering persists.
- Treatment of the cause:In cases of SALDO management should be aimed at treating the primary cause
B.Infections of the lacrimal excretory system:
Canaliculitis:
Infection of the canaliculus can be caused by a variety of bacteria, viruses, and in rare cases, fungi. The most common organism is Actinomyces Israeli.
Clinical features:
- Chronic watering with or without pain
- Conjunctivitis localized near the medial canthus
- Pouting of the puncta
- Expression of granules on milking the canaliculus
Treatment:
Topical antibiotics and irrigation of the lacrimal system with antibiotics after expressing the expressed material for culture and sensitivity. If conservative management fails, Canaliculotomy and curettage is undertaken.
Acute Dacryocystitis:
Dacryocystitis is inflammation of the lacrimal sac resulting from a complete NLD block. Clinical features of acute dacryocystitis include pain and swelling in the lacrimal sac area. The swelling is tender and erythematous. There can be lacrimal sac abscess formation, and the swelling is fluctuant in these cases. Staph aureus and Steptococcus pneumonia are the most common organisms responsible for acute dacryocystitis. Acute dacryocystitis is an ophthalmic emergency and can also lead to other complications.
Complications of acute dacryocystitis:
- Conjunctivitis
- orbital cellulitis
- Lacrimal sac abscess
- Lacrimal sac fistula formation
- Osteomyelitis of lacrimal bone
Management of Acute dacryocystitis:
- ROPLAS and irrigation of the lacrimal system is strictly avoided as it can lead to further spread of infection
- Topical and systemic antibiotics covering both gram-positive and gram-negative organisms are the treatment of choice. Parenteral antibiotics are indicated in orbital cellulitis
- Incision and drainage are done in lacrimal sac abscess. The drained pus is sent for culture and sensitivity.
- Once the acute infection has resolved the patient needs to be planned for dacryocystorhinostomy to avoid such attacks in future
Chronic dacryocystitis:
Chronic dacryocystitis is a chronic low-grade infection of the lacrimal sac resulting from long-standing NLD obstruction. The patient has complaints of watering with a discharge without pain. ROPLAS test is positive. Lacrimal sac irrigation can be done to further confirm the diagnosis, which will show complete regurgitation of mucoid fluid from opposite puncta. Patients of chronic dacryocystitis can have repeated attacks of acute dacryocystitis until the NLD obstruction is relieved by surgical intervention. Long-standing chronic dacryocystitis can lead to the formation of lacrimal sac mucocele. Complications of chronic dacryocystitis include chronic conjunctivitis, eczema and ectropion of lower lid because of persistent epiphora and wiping, and formation of mucoele and lacrimal sac fistula. Any intraocular surgery is contraindicated until the NLD block is relieved.
The surgical options are the same as described in the management of NLDO.
Lacrimal sac mucocele:
Chronic dilation with enlargement of the sac is termed a mucocele. (Fig. 13) On pressing the swelling mucoid fluid is expressed out through the puncta and the swelling becomes considerably smaller in size or totally disappears only to form again once the fluid gets collected. Sometimes due to persistent chronic inflammation, the opening of the canaliculi in the lacrimal sac gets blocked and the mucocele gets converted into anencysted mucocele. No fluid is expressed out on pressing over an encysted mucocele as the canalicular opening into the sac is blocked and hence ROPLAS is negative.
The treatment of the condition is dacryocystorhinostomy or dacryocystectomy.
C.Neoplasms of the lacrimal excretory system:
Lacrimal sac neoplasms are rare. The most common primary benign lacrimal sac neoplasm is squamous papilloma and the most common malignant lesion is squamous cell carcinoma. The lacrimal sac may be involved secondarily by extension of tumors from the surrounding structures such as lids, orbit, and nasal cavity.
Clinical features:
- Firm to hard mass in the lacrimal sac area which generally extends above medial canthal tendon (Fig. 13)
- Epiphora
- Hemolacria or bloody tears
Management:
- CT Dacryocystography (CT DCG) is done to confirm the diagnosis and extent of the tumor
- Dacryocystectomy with complete removal of the mass along with the surrounding involved structures is the treatment of choice
- Radiotherapy can be used as an adjuvant measure after surgery or as a palliative measure in extensive lesions.
D.Trauma:
Trauma may be iatrogenic in the case of scarring of the lacrimal passage after overly aggressive lacrimal probing or following orbital, craniofacial or nasopharyngeal procedures. Non-iatrogenic traumatic causes are midfacial fractures involving the bones of the nasolacrimal duct. Naso-orbito-ethmoidal fractures are an important cause of traumatic NLDO with telecanthus. (Fig. 14)
A canalicular laceration is repaired as soon as possible (within 48-72 hours) by approximating and suturing both the cut ends of the canaliculi after passing a silicone stent through them to maintain the patency. The silicone stent is generally removed after 3-6 months.
Traumatic NLD obstruction is treated by dacryocystorhinostomy with intubation.
Dacryocystorhinostomy:
Dacryocystorhinostomy is the procedure of choice for most cases with acquired NLD obstruction.
Aim of the surgery:to bypass the block in the nasolacrimal tract and create an anastomosis between the lacrimal sac and middle meatus of the nose.
Types of DCR:
DCR can be of following types
- External DCR
- Endonasal DCR
- Laser DCR
- Conjunctival DCR
External and endonasal DCR are the two most commonly formed surgeries for NLDO. External DCR is done through an incision over the lacrimal sac externally, endonasal DCR is done through nasal route and with the help of an endoscope.
Laser DCRs use the laser to form the new passage and their failure rates are high. Conjunctival DCR is done in cases of canalicular obstruction.
Success rates of both external and endonasal DCR are approximately 90-95% in experienced hands. External DCR is generally preferred by most of the ophthalmologists. The major advantages of endonasal DCR includeno visible scar, less bleeding and quicker recovery.
Pre-op Evaluation:
- Nasal endoscopic examination preferably by an otorhinolaryngologist to rule out any nasal pathology especially deviated nasal septum and atrophic rhinitis
- Routine lab investigations including coagulation profile
Surgical steps of external DCR:
- Anesthesia: External DCR is generally performed under local anesthesia except for children, traumatic NLDO and uncooperative patients where general anesthesia is preferred.
- A skin incision is given medial to the medial canthus along the anterior lacrimal crest
- Periosteum over the anterior lacrimal crest is reflected.
- The lacrimal sac is dissected from the lacrimal sac fossa and reflected laterally.
- The anterior lacrimal crest and the bones forming the lacrimal fossa is removed using a bone punch to create an ostium of 15 X 15 mm
- The nasal mucosa is exposed
- H shaped incision is given on both the lacrimal sac and nasal mucosa to create anterior and posterior flaps
- The anterior and posterior flaps of the lacrimal sac and nasal mucosa are sutured together
- The wound is closed in two layers.
Complications of external DCR:
- Intraoperative, immediate and delayed hemorrhage
- Orbital hemorrhage
- CSF leak
- Infection
- Failure of surgery
- Scar formation
Comparison of External and endonasal DCR
|
External DCR |
Endonasal DCR |
|
Advantages |
Advantages |
|
The comparatively higher success rate |
No visible scar |
|
Small learning curve |
Comparatively less bleeding |
|
Does not require any expensive instrument |
Quick recovery |
|
|
Any nasal pathology can be addressed simultaneously |
|
Drawbacks |
Drawbacks |
|
Visible scar |
Comparatively less success rate |
|
More bleeding |
Steep learning curve |
|
Injury to the medial canthus |
Requires expensive instruments |
|
More surgical time |
Further reading:
- Kanski JJ .Clinical Ophthalmology: A Systemic Approach.2007; 7th edition.66-77. Butterworth Heineman
- Albert DM, Jakobiec FA. Principles and Practice of Ophthalmology. 2008;3rd edition.3497-3501.Elsevier
- Basic and Clinical course. Section 7, Orbit, Eyelids and Lacrimal System. American Academy of Ophthalmology. 2008-2009:259–64
- Spalton, Hitchings, Hunter. Atlas of Clinical Ophthalmology.1993; 2nd Ed, Mosby Wolfe.
- Leonard A Levin, Siv F. E. Nilsson, James Ver Hoeve, Samuel Wu, Paul L. Kaufman, Albert Alm. Adler’s Physiology of the Eye: Physiology of the lacrimal system. 2011.11 edition. 350-62. Saunders