
“Cancer can take away all of my physical abilities. It cannot touch my mind, it cannot touch my heart, and it cannot touch my soul.”
Jim Valvano
Treating malignancies I believe, brings the true human spirit forward of the treating physician. Breaking the news of malignancy to a patient is as heartbreaking for the physician as it is for the patient. Yet the doctor must keep his feelings aside and do his best. Even though the human eye forms a small fraction of the human body, malignancies of all sorts and sizes can be found inside. Treatment is complex and takes a lifetime to master. In this section, I will summarize the various treatment modalities used in intraocular malignancy with a small write-up on chemotherapy and radiotherapy.
1.CRYOTHERAPY
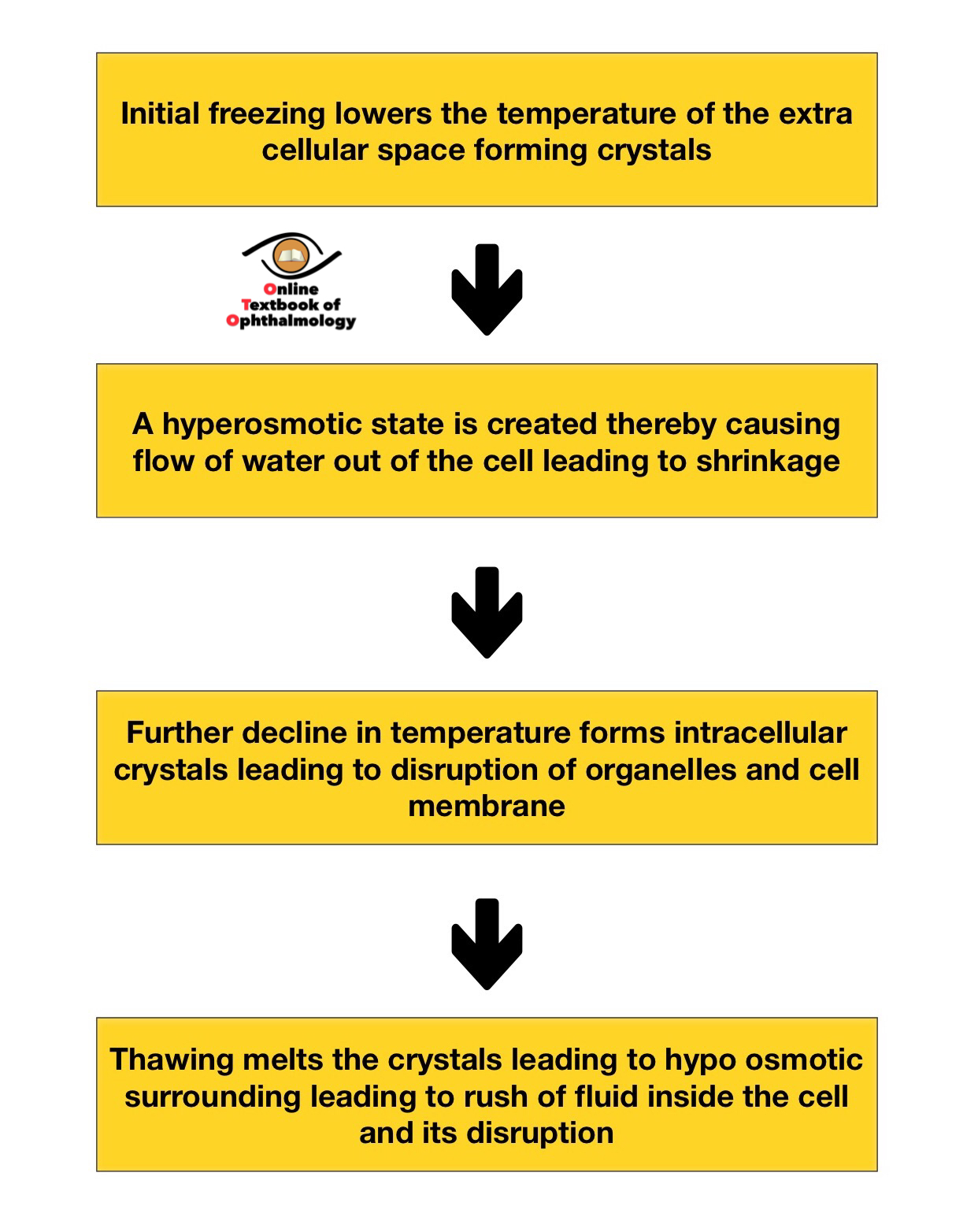
Principle of cryotherapy [1],[2]
- Direct effect
- Indirect effects:
- Initial freezing causes vasoconstriction and then the process of thawing causes vasodilation leading to increased permeability and edema
- Secondary endothelial damage leads to formation of thrombus and results in necrosis
Procedure:
- Cryotherapy is applied as a 'triple freeze thaw'technique.[1]
- Temperature close to -20 to -70 degrees celsius is generated.
- By indirect ophthalmoscopy, the peripheral lesion is lifted directly by the cryoprobe and is first frozen rapidly along with a margin of normal surrounding retina till ice formation is visible. It is then allowed to thaw slowly and naturally. The process is repeated thrice.
- The procedure can be done under local anesthesia ( in adults) or can be performed under general anesthesia
- Cryotherapy is generally reserved for lesions that are anterior to the equator.
- The procedure may need to be repeated at frequent intervals.
USES
- Retinoblastoma belonging to group A as a primary treatment when anterior to the equator
- As a consolidation treatment in Retinoblastoma for the peripheral lesion.
- It is mainly used in peripheral vascular lesions like in Coats' disease, leaking capillary angioma when small.
- Commonly used in VPT(vasoproliferative tumors) as the majority of lesions are peripheral.
Conjunctival chemosis, lid edema, pain, anterior segment reaction are some of the normal effects after treatment. Rarely vitreous hemorrhage, retinal breaks occur. Lid abnormalities like depigmentation, poliosis, scarring can occur when cryotherapy is applied close to the lid margins.
2LASER[3],[4]
The use of laser is limited in the management of intraocular malignancies restricted mainly to vascular entities and some early stages of retinoblastoma and choroidal melanoma. Melanin in RPE and choroid, Xanthophyll pigments, hemoglobin in RBC are the deciding chromophores in the selection of a particular laser.
Laser forms
- Green argon laser
- Diode laser as TTT ( transpupillary thermotherapy)
- Diode laser in PDT ( photodynamic therapy)
Argon Green Laser
- Destroys the tissue on application by photocoagulation.
- Used in retinoblastoma group A as the primary form of treatment or as consolidation therapy in peripheral lesions.
- Used in early stages of Coat's disease
- As a primary mode of treatment in vascular tumors like retinal capillary hemangioma when detected early
- In cases of choroidal hemangioma, argon laser may be employed ( although PDT is favored).
Transpupillary Thermotherapy (TTT)
Principle: In contrast to traditional laser therapy where the temperature of the targeted tissue reaches above 65 degrees, in TTT the tumor is heated below 65 degrees. A greater depth of tissue destruction is achieved by TTT as compared to a normal laser.
- TTT involves the application of low energy for a long period of time
- Generally, the diode laser is utilized for TTT
Uses
- As a primary modality in group A retinoblastomas or as a consolidation therapy post other modalities( like after chemoreduction)
- For choroidal melanomas, the TTT is used for lesions that are small and preferably away from optic disc and foveola.
- Vascular tumors like capillary hemangioma.
- Rarely VPT, small choroidal metastasis is treated by TTT.
Photodynamic therapy (PDT)
Principle: It involves the administration of a light-sensitive compound that gets rapidly absorbed inside the target tissue which when activated releases reactive oxygen molecules leading to target tissue destruction. The light-sensitive compounds are commonly known as photosensitizers; verteporfin being the most commonly used in ophthalmology.
Mechanism of accumulation inside tumor tissue [3]
- Presence of high nuclear-cytoplasmic ratio.
- A high anabolic process leads to increase accumulation.
- The high permeability of tumor tissue
The excitement of photosensitizer by appropriate light leads to photodynamic reactions of two types
- Type 1 reaction: leads to the formation of superoxide oxygen radicals.
- Type 2 reaction: leads to the formation of highly reactive singlet oxygen. Compared to superoxide, singlet oxygen radicals cause most of the effect of PDT by
- direct cytotoxic effect
- destruction of peritumoral vasculature
- induces local inflammation leading to secondary effects of tumor destruction.
The procedure involves intravenous injection of verteporfin in a dose of 6mg/m2 over 10 min. Activation of dye is by 690nm diode which begins 15 min after the injection for a period of 83 seconds for the total energy of 50J/cm2.
Uses
- In recent times it has become the preferred treatment modality for choroidal hemangioma.
- Has been actively used in choroidal metastasis [5]
- Capillary hemangiomas
- Rarely used in choroidal melanoma.
3.CHEMOTHERAPY
Before going into the details of chemotherapy it is essential to understand the basics of the cell cycle. A normal cycle consists of:
Chemotherapeutic agents can be:
Cell cycle-specific: when agents are most effective at a particular stage of cell cycle example vinka alkaloids and antimetabolites
Nonspecific: when agents are effective throughout all the stages and response is dose-related, for example alkylating agents and platinum derivatives
Various chemotherapeutic agents
Group |
Drugs |
Mechanism |
|
1)AntimetabolitesGenerally, cell cycle-specific and has 3 classes |
||
|
Folic acid antagonists |
Methotrexate |
Prevents thymidine synthesis |
|
Pyrimidine analogues |
5 Fluorouracil |
Inhibits synthesis of nucleic acids |
|
Cytarabine |
Inhibits DNA polymerase |
|
|
Gemcitabine |
Inhibits DNA synthesis |
|
|
Purine analogues |
6 Mercaptopurine |
Inhibits nucleotide biosynthesis |
|
Thioguanine |
Same as above |
|
|
2)Alkylating agentsMost effective in S phase |
Nitrogen mustards |
These agents form cross-links |
|
cyclophosphamide |
||
|
dacarbazine |
||
|
3)Heavy metals |
Cisplatin, Carboplatin |
Intra or interstrand DNA cross-links |
|
4)Cytotoxic antibioticsProduced from bacterial and fungal cultures |
Anthracyclin |
All the agents affect the functioning and |
|
5)Vinca alkaloids |
Vincristine |
Binds to tubulin inhibiting spindle formation and prevents mitosis |
|
6)Topoisomerase inhibitorsPhase specific: acts between G2 and S phase |
Topoisomerase 1 inhibitor: Topotecan |
Breakage of strands and inhibits DNA replication |
Concept of Fraction Kill
A fixed reduction in the population of tumor cells with successive cycles of chemotherapy. This forms the basis of giving chemotherapy in cycles which also allows normal tissue turnover.
Chemotherapy in retinoblastoma
Few important terminologies
Adjuvant Chemotherapy: when chemotherapy is used as an adjuvant after some other form of primary treatment mainly when high-risk features are detected during histopathology to prevent metastatic death.
Neoadjuvant chemotherapy: When chemotherapy is used before other forms of definitive treatment to reduce the tumor burden.
ROUTES OF CHEMOTHERAPY IN RETINOBLASTOMA [6]
INTRAVENOUS: used mainly in unilateral or bilateral cases, familial cases, eyes with high-risk features detected on histopathology. Intravenous use of chemotherapy helps in
- effective tumor control
- prevents metastasis
- reduces the incidence of trilateral retinoblastomas
- reduces the incidence of long-term second cancers.
Agents most commonly used are Vincristine, etoposide, carboplatin(VEC)
INTRA ARTERIAL: An exciting and comparatively new modality of chemotherapy, results have been quite promising.
The procedure involves administering chemotherapeutic agents selectively into the ophthalmic artery via transfemoral route thereby delivering higher amounts of drug directly into the eye, hence calledsuper selective intraarterial ophthalmic artery chemotherapy.
The idea is to have maximum effect on the tumor without having any ill effects of the treating agent on the general body. Currently, its use in retinoblastoma is in
- Non-germline/familial cases
- Mainly Unilateral retinoblastomas
- Recurrence post-primary treatment
- For subretinal and vitreal seeds
Melphalan is the most common agent used for the intraarterial route. Although the intraarterial route appears promising in globe salvage for advanced cases, the procedure needs a team specifically trained in such maneuvers.
PERIOCULAR: This route provides chemotherapeutic agents for a long period of time at a higher dose compared to the intravenous route. Carboplatin and topotecan are the agents most commonly used.
- used in bilateral group D or E where a higher dose of systemic chemotherapy would be needed
- in the recurrent localized tumors.
The periocular route has been less popular in view of complications like fat atrophy, fibrosis of muscles, and optic atrophy.
INTRAVITREAL ROUTE: Once considered a crime, the intravitreal route has become a common route for tumor control. Its uses in retinoblastoma has been in
- Recurrence of vitreal seeds after primary treatment
- Non-responsive vitreal seeds to standard treatment
Melphalan is the most common agent used, although the use of methotrexate has also been reported.[7]
The number of injections varies from 3-6 depending on the response for melphalan. When methotrexate is used, injections are given in 3 phases( induction, consolidation, and maintenance) [7]
Important safety measures are employed during an intravitreal procedure to diminish tumor spread.
- Use of a 32 /30 gauge needle
- Aqueous aspiration prior to intravitreal injection to prevent reflux of malignant cells
- Use of cryotherapy at the injection site
- Flooding the whole eye with distilled water:Death by water.It works on the principle that retinoblastoma cells become non-viable after 2-3 minutes in an environment of distilled water.[8]
4. RADIOTHERAPY [2,9,]
Principle: Energy created in the interaction between electrons, protons, and neutrons amongst each other forms the basis of the treatment in any malignancy. The energy released can be α particles( helium nucleus), β particles (electrons) or? rays( having no charge). The energy released is in the form of ions that interact with DNA causing damage leading to impairment in cell division.
Bragg's peak or curve plots the energy loss of ionizing radiation during its travel through a particular media. The concept of Bragg's peak is utilized in proton beam therapy of cancers where high energy is delivered to the target tissue with minimal surrounding damage to normal tissues.
Radiation absorbed dose is expressed in terms ofgrays(Gy). Centigray( cGy) is commonly used in radiation therapy and it represents 1/100 of gray ( 1 cGy=1 rad) Fractionation: Delivery of radiation in multiple fractions over a number of days is termed fractionation. The purpose of such is to minimize radiation adverse effects.
Forms of radiation therapy used in intraocular malignancy
A)Brachytherapy:
The use of radiation in form of plaques that are placed adjacent to the tumor is called brachytherapy. Plaques are carriers of radioactive substances. Commonly used sources of radiation are
- Iodine 125
- Ruthenium 106
- Palladium 103
- Strontium 90
- Caesium 131
The most commonly used radioactive materials are Iodine and Ruthenium, although other radioactive materials are also used depending on the center. Plaques used in brachytherapy are
- COMS (Round ) plaque which are iodine-based plaques differing in sizes depending on the size of the tumor. The plaques have a carrier portion that has iodine seeds embedded with eyelets for suturing to the sclera.
- Notched plaques: These plaques are similar to the round one except having a slot that serves a purpose to be near the optic nerve.
- Slotted plaques: Plaques having slot built-in for passage of optic nerve for tumors involving the optic nerve.
- Gold is the carrier material for iodine-based plaque whereas silver is used for ruthenium.
Important considerations before brachytherapy
- Brachytherapy involves collaboration between a treating ophthalmologist, radiation oncologist, and a physicist for determining accurate dose as required.
- Preoperative assessment is absolutely essential for determining accurate tumor dimensions which decides the radioactive material to be used. Clinical examination, ultrasound sonography, and fundus imaging form the basis of preoperative planning.
- Ruthenium is generally employed for tumors up to 6mm thickness, iodine plaques are used in tumors with larger thickness and diameter.
- Surgery can be performed under local or general anesthesia.
- Depending on the dose, plaques are removed between 3-5 days.
Uses
- Uveal melanoma. Melanoma of the iris, ciliary body, and choroid are treated effectively by this method which forms the cornerstone of such tumors. Radiation material and size depend on the size, location, and other associated features of the tumor. The dose generally used is in the range of 70-100 Gy with the goal being the maximum dose to the tumor apex.The use of brachytherapy with TTT in treating uveal melanomas is called Sandwich therapy
- Retinoblastoma: Although not used commonly as primary therapy, it is useful for cases of residual or recurrent localized tumors. Vitreous seeding is a contraindication for use of plaques in retinoblastoma.
- Vascular lesions like choroidal hemangioma, retinal capillary hemangioma, VPT are also treated with brachytherapy
Contraindications for radiation therapy
- Tumors with large extra ocular extension(>5mm). Localized extraocular metastasis or distant metastasis is not a contraindication.
- Painful blind eyes are better treated with enucleation.
- Patients whose death is imminent.
- Patients are not fit for a surgical procedure
B)PROTON BEAM THERAPY
- Mode of radiation delivery by means of charged protons .
- Used in choroidal melanomas which are large for brachytherapy or in cases where the lesion is posterior located
- Also used in choroidal hemangiomas, iris melanomas.
- The dose is generally 60 Gy fractionated over 4 days.
- Avoided in cases with extensive extraocular metastasis, or tumor which are large enough to cause treatment-related complications.
C)STEREOTACTIC RADIOTHERAPY
Involves delivery of a precise dose of radiation with minimal surrounding tissue damage. It can be
- Stereotactic radiosurgery: use of multiple radiation beams from different directions. This modality incorporates a Gamma knife which is a radiation delivery module comprising of cobalt.
- Fractionated stereotactic radiotherapy: use of a single beam of radiation from multiple directions. A linear accelerator is used for the same
Its use is restricted to choroidal melanomas which are either too large or posterior for brachytherapy.
D)EXTERNAL BEAM RADIOTHERAPY
Once a common method of treatment for retinoblastoma, its use has drastically reduced, and rightly so. It was realized children receiving EBRT especially those below 1 year were prone to develop non-ocular malignancies in the future. Hence there exist few indications for EBRT like residual orbital disease after enucleation for retinoblastoma.
Complications of radiotherapy: Complications are listed in general and it depends on the dose and form of treatment.
Early
- Lid edema, erythema, and crusting
- Conjunctivitis and discharge
- Acute exudative retinal detachment
- Choroidal detachment
- Corneal punctate changes especially when used for iris and ciliary body lesions.
Late
- Lid anomalies
- Dry eye and lacrimal gland atrophy
- Canalicular obstruction
- Dry eye and secondary corneal changes
- Cataract
- Scleral thinning.
- Radiation retinopathy: occurs 2-3 yrs after treatment
- Radiation neuropathy: occurs 1-3 yrs post-treatment
- Chronic retinal detachment
- Neovascular glaucoma
- Temporal bone anomalies: with EBRT
- Secondary malignancies: with EBRT
5.SURGICAL INTERVENTION
- Iridectomy: reserved for lesions of iris less than 4 clock hours and not involving the angle.
- Iridocyclectomy: for lesions of iris and ciliary body < 1/3. Melanoma, adenocarcinoma of the iris, and ciliary body can be treated by this approach.
- Resection of choroidal melanoma
- Exoresection: The tumor in toto is resected by creating a partial thickness scleral flap. It is employed as a primary modality in cases seemed too large for radiotherapy or as a salvage procedure after radiotherapy to remove the active tumor when the patient denies enucleation.
- Endoresection of a choroidal tumor is a controversial subject practiced by very few surgeons. In principle, it involves the removal of the choroidal tumor by a pars plana approach. It can be used as a primary modality of treatment for cases not fit for radiation. More commonly this method is employed in cases after radiotherapy in treating cases having associated retinal detachment.
Both the resection techniques can provide great results in expert hands but need years of practice.
Enucleation: is the treatment of choice when the eye seems unsalvagable.
- It is the treatment of choice for eyes having advanced group E and diffuse variety of retinoblastoma disease
- In eyes with obvious extraocular spread use of chemotherapy as an adjuvant /neoadjuvant therapy is mandated.
- It is the treatment of choice for choroidal melanoma with advanced disease.
- Enucleation is again favored in cases where the clinical possibility of tumor cannot be ruled out
References:
1) ShieldsJA, Parsons H,ShieldsCL, Giblin ME. Theroleofcryotherapyin the management of retinoblastoma. Am J Ophthalmol.1989 Sep 15;108(3):260-4.
2) Singh AD, Damato BE, Pe'er J, Murphee AL, Perry JD. Clinical Ophthalmic Oncology .Philadelphia: Saunders, Elsevier 2007
3) Cerman E,Cekic O. Clinicaluse ofphotodynamictherapyinoculartumors. Surv Ophthalmol.2015 Nov-Dec;60(6):557-74
4) Lingam G. Options for management of intra ocular tumors. Indian J Ophthalmol.2015 Mar;63(3):204-10
5) Kaliki S, Shields CL, Al-Dahmash SA, Mashayekhi A, Shields JA. Photodynamic therapy for choroidal metastasis in 8 cases. Ophthalmology. 2012;119:1218–22
6) Shields CL,Lally SE,Leahey AM,Jabbour PM,Caywood EH,Schwendeman R, et al. Targetedretinoblastomamanagement: when to use intravenous, intra-arterial, periocular, andintravitreal chemotherapy. Curr Opin Ophthalmol.2014 Sep;25(5):374-85
7) Kivelä T,Eskelin S,Paloheimo M. Intravitreal methotrexate for retinoblastoma. Ophthalmology.2011 Aug;118(8):1689, 1689.e1-6
8) Francis JH,Xu XL,Gobin YP,Marr BP,Brodie SE,AbramsonDH. Deathbywater: precautionarywatersubmersion for intravitreal injection of retinoblastoma eyes. Open Ophthalmol J.2014 May 16;8:7-11
9) Damato BE. Ocular Tumours. Diagnosis and treatment. Butterworth-Heinemann 2000