
1. Suspect :
Any unusual post-operative reaction ( out of proportion to surgical trauma ) should be suspected for Endophthalmitis.
2. Differentiate from TASS :
All unusual post-operative reactions may not be infective; Pointers towards Toxic Anterior Segment Syndrome could include: Early onset of Limbus to limbus corneal edema with good fundus glow and no exudates in the vitreous cavity. The presence of Lid edema, chemosis, a marked reduction in vision, vitreous exudates, and low intraocular pressure should alert one for Infective Endophthalmitis.
3. Talk :
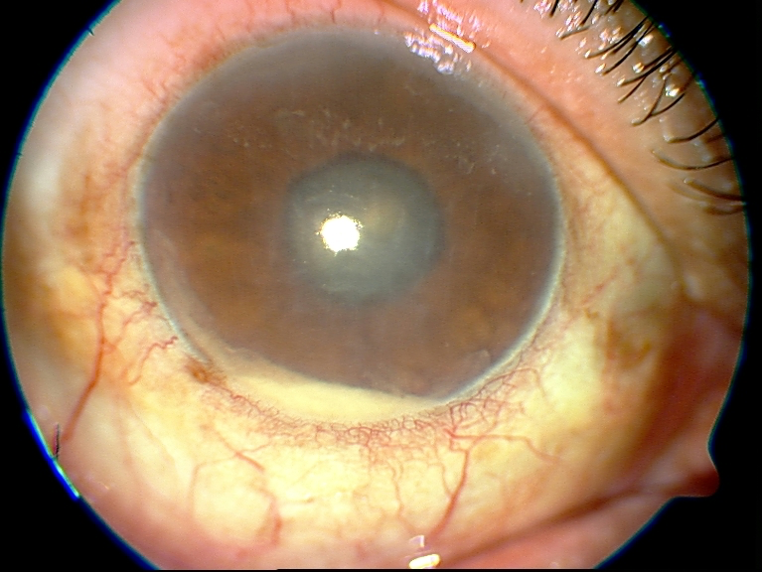
The most difficult part is how to tell the patient about this. This is a very sensitive issue because in Today`s time, no patient is willing to take any negative news ( Thanks to Trivilisation of eye surgery / googlisation etc.) and there is always a potential for medicolegal issues cropping up. Talking requires some degree of compassion. It is advisable to take a picture of the anterior segment & fundus, even if hazy. Take patient & relatives to a separate room – Explain to all .. what the picture looks like & how should the normal be. Discuss with patients & all relatives that any cut / any surgery has the potential to have an infection, despite the best precautions. This can happen in the best of setups, anywhere in the world.
Talk & Talk :
Also, explain that all is not lost & it is possible to have recovery in most of these patients. This can have a calming effect on the patient, who was expecting to join back his work, with full vision. Tell him & family that you will make the best possible efforts to help him recover and you won`t be charging additional fees for your services.
4. Peer Review :
If you are a VR surgeon, shouldn’t be much of a challenge, although it may be better if a senior surgeon in your setup, if any, also sees the patient & is kept in the loop – this will assure the patient & more importantly his relatives that the best possible is being done for the patient. If you are an Anterior segment surgeon, you can have an opinion from a VR colleague within your setup. If however, VR help is not there in your setup.. the best is, if you are confident ( which all ophthalmologists should be ) to give an intravitreal antibiotic injection & seek an urgent VR opinion.
5. Prompt Intravitreal Injection:
If the diagnosis of Endophthalmitis is confirmed / there is a high index of suspicion, prompt intravitreal Antibiotic Injection should be given without delay ( even if it is a holiday ). It is always better to give 2 antibiotics, one for Gram-positive organisms & the other for Gram-Negative organisms. The usual recommendation is Vancomycin + Ceftezidime; If suspicion for Gram-Negative is high: Can give Vanco + Amikacin (taking care of dilution errors ); For a very severe Endoph, Can give Tazobactum & Piperacillin. If a clinical picture/ KOH smear suggests Fungal Endophthalmitis, could add Voriconazole in the intravitreal injection.
6.Regular / Daily Review:
If the clinical diagnosis is TASS and patient has been put on intensive steroids, cycloplegics, etc .. it is imperative to review the patient in the evening .. if improvement – can continue medical treatment & review the next day, then daily. If intravitreal antibiotics have been given, then you can see the next day for signs of improvement/stabilization.
7.Culture Report :
Once it has been decided to give intravitreal antibiotics / take up the patient for Vitrectomy, it is desirable to take samples for culture & sensitivity. The best yield is with vitreous biopsy. Alternatively, aqueous paracentesis can be done. Inoculation of samples should be done in the operation theatre itself.
8. Early Vitrectomy:
If a patient doesn`t respond at all to intravitreal antibiotics in 24-48 hours or if endophthalmitis is very severe with PL vision, pars plana vitrectomy should be done. Other indications of Vitrectomy could include: Retained Intraocular Foreign body, Recurrent Endophthalmitis, Retinal detachment on Ultrasound.
9. Referral to Higher Centre :
If the patient is not responding adequately o your treatment / If the surgeon is not confident of doing a Vitrectomy ( whenever needed ) / if facilities for Vitrectomy are not available, the patient should be referred to a higher center urgently.
10. Document & Document:
Whatever are the findings, please write them in the case sheet, preferably with a drawing and photographs. Also very important is to write down your plan of action & the discussion you had with the patient & relatives. The details of every treatment given smears made, cultures sent should all be recorded with date & time. Remember it is this documentation which is going to help you in court of law (if litigation issues arise ). Also remember, what matters in the court of law is that you have tried your best & given the best possible treatment and not the result. If there is an issue of Cluster Infections, review all the patients operated on the same day(s), review all sterility factors for any breach in protocol & Inform health authorities & AIOS, apart from treating/referring all patients