
Phacoemulsification of the very dense cataract presents the surgeon with a series of specific and difficult challenges.How hard is hard and what level of hardness makes it challenging depends largely on the experience of the surgeon. LOCS III classification does not always reveal the real hardness of the cataract, and that aside there is no definition in the literature that classifies the hardness of cataract. A hard cataract is a relative term relative to the surgeon’s experience and confidence!
I have over the years put some criteria for myself when I call it a difficult situation. These are dark brown to the black nucleus, no visibility of the posterior slit beam due to the nuclear sclerosis, an older patient, diabetic patient, and preoperative poor vision. Ocular co-morbidities such as pseudo exfoliation, absence of pupillary ruff and calcific spots on the anterior capsule are some of my personal markers which add further to an already challenging surgery
Pearl 1: Preoperative considerations
A detailed slit lamp examination keeping the above-mentioned points in mind is mandatory. Absence of pupillary ruff even if the pupil dilates well during the preoperative slit-lamp examination, relative anterior microphthalmos and phacodonesis should alert the surgeon to a possibility of a rough time in the theatre. History regarding medication, especially the use of Tamsulosin should be noted. Endothelial assessment must be thorough, specular microscopy must be done if required. Optical biometry is preferable but, if difficult, immersion A scan can be done with equally good results. Chair time is important, patients must be explained about the higher probability of complications irrespective of skill and experience of the surgeon.
Pearl 2: Anaesthesia/Approach
Peribulbar, parabulbar or topical, depends not only on surgeon’s comfort and experience but also on patient’s ability to cooperate for a possibly longer surgery. In situations where pupillary dilation is inadequate, it may be better to do the surgery under peribulbar anaesthesia. There should be no ego during surgery and both patient and surgeon must be comfortable.
I always perform phacoemulsification from the temporal approach ( 0 or 180 degrees), this approach gives more room to maneuver the probe even in deep-set eyes. I always make a clear corneal entry, however, a word of caution here is not to make the wound too long, as it increases the chances of oar locking of the probe and increases the possibility of corneal burns. Alternatively, a sclero-corneal tunnel can be created which makes the conversion to manual sutureless surgery easier should the need arise.
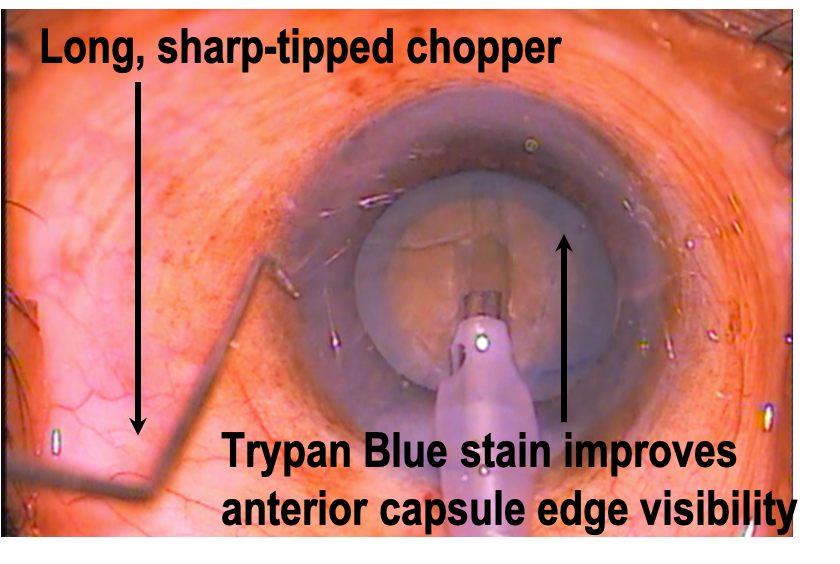
Pearl 3: Staining the capsule
Poor fundal glow makes capsular visualization difficult, and staining is an important adjunct to make complete and adequate sized rhhexis. Secondly anterior capsular edges are better visualized when stained with trypan blue during chopping procedures, preventing the chances of an inadvertent tear.If high intra-lenticlular pressure is present, it warrants lens decompression before completion of the rhhexis.
Pearl 4: Ocular viscoelastic device (OVD)
The endothelium needs additional protection compared to routine phacoemulsification. Cohesive viscoelastic (Sodium Hylauronate 1% or more) alone is good to create space but does not coat well and gets washed away very easily. A dispersive viscoelastic which coats the endothelium and is relatively more retentive is preferred, hence the need for a Sodium Hyaluronate(30mg) + Sodium Chondroitin Sulfate(40mg) combined OVD (VISCOAT).To minimize resistance in the manipulation of instruments and during capsulorrhexis balanced salt solution or methylcellulose can be injected on the lens surface, thereby pushing the Viscoat towards the endothelium. Alternatively, a visco-apdaptive OVD can be used below the dispersive OVD. These principles are based on the soft-shell techniques described by Steve Arshinoff.
Pearl 5: Hydro-procedures
Cortico-cleaving hydrodissection should be performed as described in the literature. The posterior lip is depressed to express out some OVD before beginning the hydrodissection. The cataract being voluminous occupies the bag in its entirety. There is very little epinuclear cushion. The fluid wave cannot be visualized due to the compactness of the cataract. The sign of a subtle anterior movement of the cataract confirms the passage of the fluid wave, but caution must be exercised at this point in pursuing with the hydro procedure as the fluid may get trapped between the cataract and the posterior capsule and cause posterior capsular dehiscence. The center of the nucleus must be gently depressed with the shaft of the hydro-canula to express the fluid out and terminate the capsulo-lenticular block. Hydro-procedure can then be repeated in a similar manner if required. A Sinskey’s hook can then be used to gently try and rotate the nucleus confirming a good hydro-dissection
Pearl 6: Nucleus management
The most worrisome of the steps. Leathery, hard nucleus therefore difficult to chop, lack of epinuclear layer, reports of the thinner capsule, and the possibility of weaker zonules, all make it challenging.
The 3 key steps - debulk, chop and sub-chop
I always create a crater or wide and deep groove before beginning to chop. This gives the additional space to stay away from the endothelium and helps impale at a deeper plane. Low vacuum and high power, continuous power delivery settings are used. The wide groove is made till the fundal glow is better visualized before initiating the vertical chop.
I prefer vertical chopping and it works best with a long (1.25 or 1.5mm) and sharp tip chopper. High vacuum, moderate power in burst mode helps to impale the phaco tip in the substance of the nucleus at a deeper plane. The h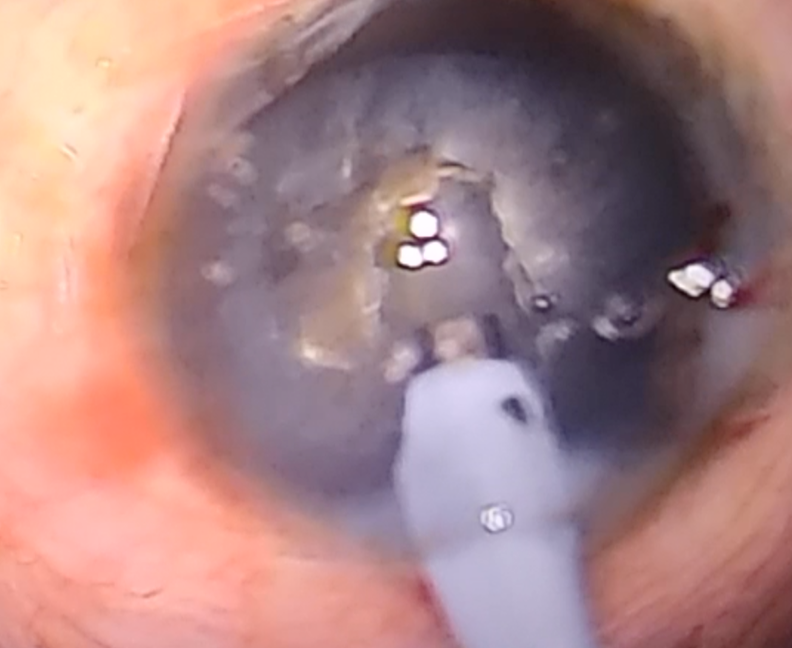 and with the chopper moves down through the substance of the nucleus, while the phaco tip stays buried in the nucleus with the foot in maximum vacuum position, and moves up and lateral causing the vertical split, however, the leathery nature may prevent separation of the posterior plate. It is crucial to ensure this separation. This can be done by re-grasping the nucleus at a deeper plane, just anterior to where the crack has extended, and repeat the same chopping manoeuver until a full-thickness crack is achieved. Rotate the nucleus and complete the chopping procedure, to get 6 or more “pies” before beginning the emulsification, keeping the pies in place helps further chopping.
and with the chopper moves down through the substance of the nucleus, while the phaco tip stays buried in the nucleus with the foot in maximum vacuum position, and moves up and lateral causing the vertical split, however, the leathery nature may prevent separation of the posterior plate. It is crucial to ensure this separation. This can be done by re-grasping the nucleus at a deeper plane, just anterior to where the crack has extended, and repeat the same chopping manoeuver until a full-thickness crack is achieved. Rotate the nucleus and complete the chopping procedure, to get 6 or more “pies” before beginning the emulsification, keeping the pies in place helps further chopping.
Key pointshigh vacuum, burst mode, impale deep, persist with the vacuum to “hold” the nucleus, separate the posterior plate by repeating the procedure.
Pearl 7 - Emulsification
Whether peristaltic or venturi, a thorough understanding of the fluidics and the settings is crucial. High vacuum, proportionately high flow rate (in peristaltic machines), moderate power, and use of hyper pulse while emulsifying the chopped pieces prevents chatter and ensures good follow ability. Torsional or transversal ultrasound delivery if available is beneficial.
Emulsification within the central crater or at the pupillary plane is safe. Dispersive OVD may have to be replenished and used as a buffer as the last few pieces are removed. Dispersive OVD better resist aspiration and prevent the trampolining of the posterior capsule.
Horizontal sub- chopping helps easier emulsification of the smaller nuclear fragments.
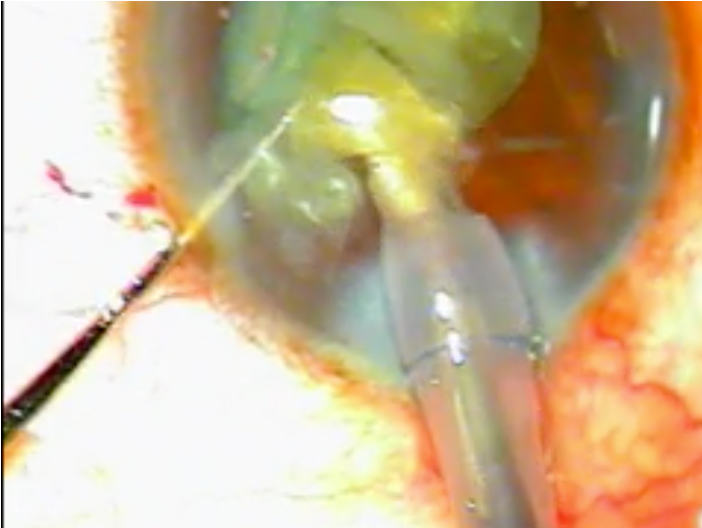
Do not leave the port un-occluded while in vacuum. Here the iris is caught in the port as the nuclear piece is being emulsified
Pearl 8: Signs to stop and review
Signs to stop and review - Cataract “milk" or phaco “smoke” may be seen which is common as the dense nuclear pieces may clog the outflow. Secondly the “heavy viscoelastic” may also block the port of the phaco tip, persisting with phaco at this stage causes heat to build up resulting in corneal wound burn.It is best to stop emulsification at this juncture, recheck inflow and outflow and restart the procedure.
Small pieces should be dealt with immediately as they may lodge in the sulcus, angle or in the subincision space and cause severe inflammation.
Decrease the vacuum as the remaining pieces decrease. Use dispersive viscoelastic to inflate the bag and act as a buffer while emulsifying the last 2 or 3 pieces.
Pearl 9: Be prepared for all eventualities.
Use a CTR if zonular stability is in doubt. Capsule supporting hooks and iris retractor hooks may also be needed if the pupil comes down after manipulation.
Pearl 10: Do not hesitate to “bailout” by converting to conventional large incision surgery if and when required.
Do not hesitate to “bailout” by converting to conventional large incision surgery if and when required. Pupillary snap sign, sudden deepening of the anterior chamber, tilting of the entire nucleus, an area of extra clarity, sudden stoppage of phaco as vitreous and nuclear piece clog the phaco tip are ominous signs, it is important to recognize them and stop phacoemulsification to reconsider the next step As I said earlier there is no shame in calling for help or in changing the approach as the best surgeons always remember that they are operating on a person and not dealing with just the nucleus.