


Introduction
Choroidal neovascularization(CNV) or choroidal neovascular membrane (CNVM) is a growth of new choroidal vessels into the subretinal space through breaks in the Bruch's membrane. Ophthalmoscopically the CNVM appears as a greenish-grey lesion, often with a detachment of the sensory retina, subretinal blood, and exudates. Choroidal neovascularization can be multifactorial with the commonest being due to age-related macular degeneration (AMD), called the wet or exudative AMD. The other causes of include high myopia, angioid streaks, presumed ocular histoplasmosis syndrome, choroidal rupture post-trauma, osteoma, macular telangiectasia, inflammatory and idiopathic.
Since the most common cause of CNVM remains age-related, this writeup will focus on the same. Age-related macular degeneration is the most common cause of blindness in the western world over the age of 65 years. With a worldwide UN estimate of about 20-25million, 8 million individuals are in the USA alone.1 The number of people suffering from AMD worldwide is around 196 million currently, and estimated to increase to 288 million in 2040.3 AMD can be classified into two forms, a dry or non-neovascular and wet or neovascular type. The dry AMD causing gradual vision loss due to changes in the retinal pigment epithelium (RPE), drusen, and atrophic changes and worsens to visually debilitating geographic atrophy. The exudative or neovascular form of AMD is a leading cause of severe vision loss in the elderly if left untreated and it accounts for up to 10% of AMD cases.2,4 The risk factors include drusen, RPE alterations, visible light injury, cigarette smoking, family history including genetic predisposition, cardiovascular risk factors (including systemic hypertension), aspirin usage, and cataract surgery.4 While, AMD is a multifactorial disease, it has a strong genetic component. Early studies have examined alleles shared between siblings, a meta-analysis of six such studies found evidence of susceptibility loci, notably at 1q and 10q26. Many of the genetic alterations found on chromosome 1 reside in genes encoding components of the complement cascade, part of a host’s innate immune system. In 2005, four separate studies examined SNP associations and found that variation within the CFH gene on chromosome 1 represented the most significant predisposition for AMD. A point mutation, rs1061170, was identified as the susceptibility allele. FH and ARMS2/HTRA1 alleles represent the most influential of all the genetic factors contributing to AMD, and together they increase AMD predisposition by more than 40 times.5
Pathogenesis
The pathophysiology of AMD is complex, multifactorial, and poorly understood and postulated to be a result of a complex multifactorial interaction between metabolic, functional, genetic, and environmental factors.7 (Figure 1)With aging, intracellular residual bodies containing lipofuscin accumulate in RPE cells.8 Thickening of BM, accumulation of lipofuscin granules in the RPE, and choroidal vascular changes have also been recorded with age in the human macula in eye bank eyes.9, 10 A gradual RPE dysfunction results in the inability of RPE and choriocapillaris to eliminate by-products of metabolism and this results in alterations in the permeability of Bruch’s membrane, which leads to an accumulation of extruded material (drusen) between the two layers.8 (Figure 2)AMD also is documented to have thinning of choriocapillaris, which may contribute to the further decline in the removal of extracellular material that results in drusen formation.11
The CNVM appears as a neovascular sprout growing under or through the RPE via breaks in Bruch’s membrane12 Several pro-inflammatory and pro-angiogenic factors like fibroblasts, myofibroblasts, lymphocytes, macrophages13 and vascular endothelial growth factor (VEGF)14 aid in the advancing inflammatory cascade and eventual neovascularization. Following penetration of the inner aspect of Bruch’s membrane, the new vessels proliferate laterally between the RPE and Bruch’s membrane.12 As these neovascular twigs mature, they develop a more organized vascular system stemming from a trunk of feeder vessels of the choroid, as well as the proliferation of fibrous tissue. (Figure 3)
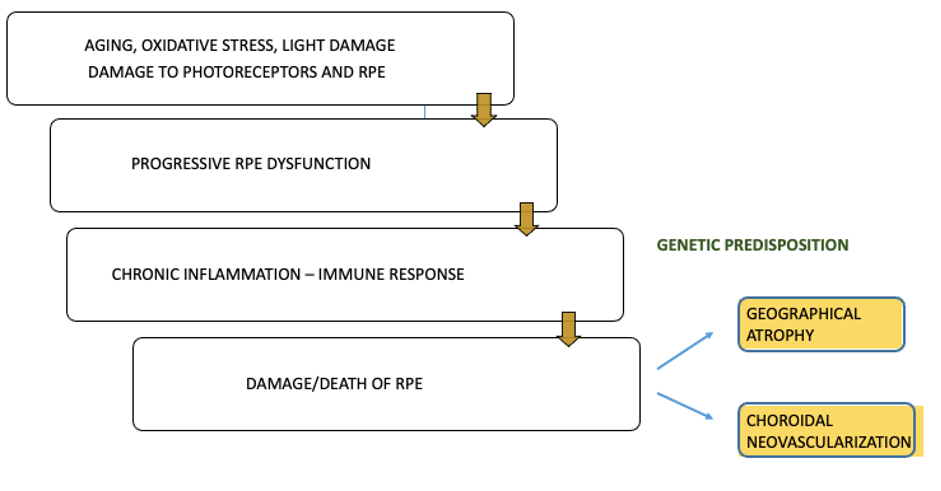
Figure 1 Pathomechanism of AMD
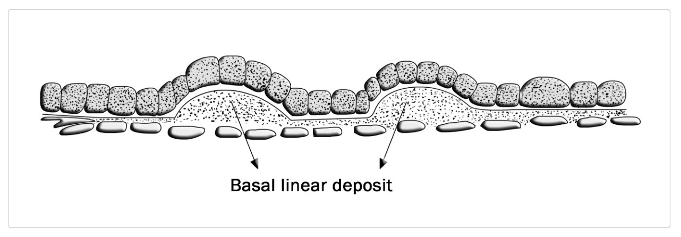
Figure 2 Development of basal linear deposits
Multifactorial pathogenesis of advanced AMD
The inflammation angle
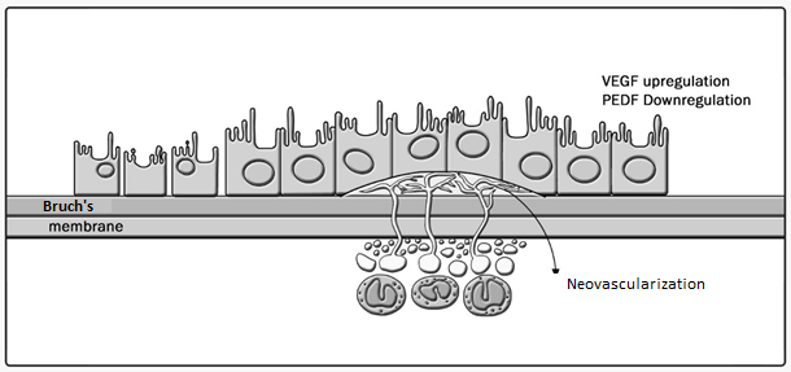
Figure 3CNVM development in relation to the RPE
Hypoxia and aging causing A2E (Lipofuscin fluorophore) and ultimate effect of wet transformation in the centre. The picture also depicts an interplay between angiogenic and antiangiogenic factors like PEDF. VEGF release mechanisms and resultant hyperpermeability with eventual angiogenesis. (Figure 4) VEGF increases in hydraulic conductivity of isolated microvessels that are mediated by increased calcium influx and likely changes in levels of nitric oxide caused by induction of nitric oxide synthetase.
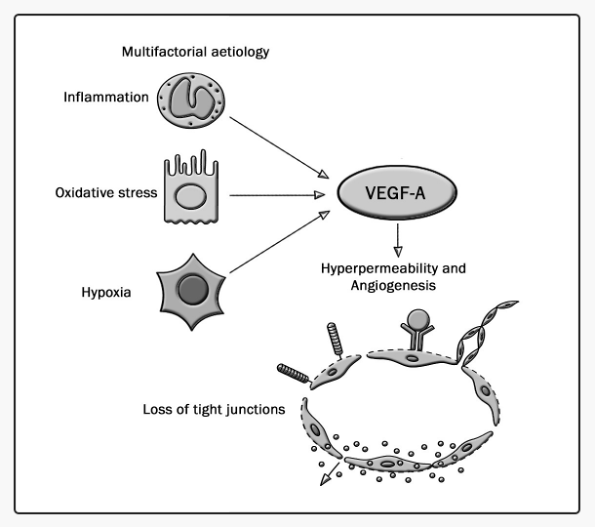
Figure 4Multifactorial etiology in the breakdown of the blood-retinal barrier(BRB) and Angiogenesis
Angiogenic factors in choroidal neovascularization
A brief outline of the Angiogenic factors in CNVM16-19
- Vascular Endothelial Growth Factor (VEGF) is the principal factor responsible for neovascularization. The primary methods of VEGF action include increased vascular permeability and then angiogenesis. VEGF is primarily secreted by Choroidal endothelial cells, macrophages, and stromal RPE. VEGF165 is the main isoform involved in pathologic neovascularization. VEGF acts through two receptor tyrosine kinases (RTKs) VEGFR-1 and VEGFR-2. VEGFR-1 is upregulated by a hypoxia-inducing factor (HIF). VEGFR-2 binds VEGF with lower affinity compared to VEGFR-1 but is the major mediator of the mitogenic, angiogenic, and permeability enhancing effects of VEGF. Other inducers of VEGF include bFGF, TGF-ß, and AGEs.16-19
- Basic Fibroblast Growth Factor (bFGF) – bFGF is heparin-binding proteins found in normal retina and RPE. bFGF and VEGF act together and are known to be the signaling factors in angiogenesis.16-19
- Advanced Glycation End-products (AGEs) – Nonenzymatic protein glycation end products. Localized in deposits and drusen and Induce VEGF expression by RPE and promote Lipofuscin formation.16-19
- Angiopoietins: Specific to endothelial cells. Act through the Tyrosine kinase receptor. Two isoforms are known. Angiopoietin 1 is more balancing with a stabilizing and non-leaky role, promotes vascular integrity (endothelial-specific growth factor). Angiopoietin 2 is upregulated by hypoxia and VEGF and results in neovascularization.16-19
- Pigment Epithelial Derived Factor (PEDF) is abundantly produced by RPE cells, is strongly anti-angiogenic, and induces endothelial cell apoptosis. The mode of action is through inhibition of VEGF receptor signaling and low levels of PEDF have been noted in cases of CNVM.16-19
- Platelet-Derived Growth Factor (PDGF) is a glycoprotein essential in the maintenance and survival of new vessels acting through 2 receptor isoforms PDGFR-A and PDGFR-B. Plasticity window, when pericyte coverage is complete, new vessels get resistant to VEGF withdrawal.16-19
AREDS classification: 21, 22
Based on drusens presence, size, and RPE alterations at the macula, AMD was classified into Early, Intermediate, and Advanced/Late AMD.
|
CLASSIFICATION OF AMD |
DEFINITION |
|
No apparent aging changes |
No drusen and no AMD pigmentary abnormalities |
|
Normal aging changes |
Only drupelets (small drusen <63mm) and no AMD pigmentary abnormalities |
|
Early AMD |
Medium drusen >63mm and <125mm and no AMD pigmentary abnormalities |
|
Intermediate AMD |
Large drusen >125mm and/or any AMD pigmentary abnormalities |
|
Late AMD |
Neovascular AMD and/or any geographic atrophy |
Table 1 Classification of AMDAMD – age-related macular degeneration. Lesions assessed within 2 disc diameters of the fovea in either eye. AMD pigmentary abnormalities = any definite hyper or hypo pigmentary abnormalities associated with medium or large drusen but not associated with known disease entities.
|
BECKMAN |
DEFINITION |
AREDS simplified score |
AREDS classification/ categories |
|
No apparent aging changes |
No drusen and no AMD pigmentary abnormalities |
0 |
No disease |
|
Normal aging changes |
Only drupelets (small drusen ≤63mm) and no AMD pigmentary abnormalities |
0 |
No disease or early stage |
|
Early AMD |
Medium drusen >63mm and ≤125mm and no AMD pigmentary abnormalities |
0 |
Early or Intermediate |
|
Intermediate AMD |
Large drusen >125mm and/or any AMD pigmentary abnormalities |
1-4 |
Intermediate |
|
Late AMD |
Neovascular AMD and/or any geographic atrophy |
n/a, 5 |
Advanced |
Table 2Comparison of AREDS and Beckman system of AMD classificationNew Beckman Staging of age-related macular degeneration and how it compares to Age-Related Eye Disease Study (AREDS) simplified grading scores and AREDS classification
Clinical features
Patients can present with a sudden or gradual blurring of central vision. The other symptoms include metamorphopsia, central scotoma, and the slow recovery of visual function after exposure to bright light. A CNVM can have a varied morphological presentation
- Pigment Epithelial Detachment (PED) with Intraretinal (IRF) and or Subretinal fluid (SRF)
- PED associated with hemorrhage which may be subretinal, preretinal or vitreous
- Retinal and subretinal cicatrization (disciform scar) in an evolved or treated lesion.
- Intra and subretinal lipid deposition
- Exudative retinal detachment, which may be extensive, resulting in total visual loss
- RPE rip
Investigations
Routine investigations that are done in the case of CNVM include color fundus photo, an SDOCT, fundus fluorescein angiography (FFA), indocyanine green angiography (ICGA), and OCT- angiography (OCTA), which is a non-invasive method of visualizing the retinal and choroidal blood vessels.
Optical Coherence Tomography (OCT)
OCT is a non-invasive and irreplaceable rapid imaging method of diagnosing and monitoring macular pathologies. OCT, a spectral-domain (SD-OCT-840 nm with 50000 A-scans/sec) as well as a swept-source (SS-OCT-1050nm with 100000 A-scans/sec)providescross-sectional imaging of the macula revealing the intricate details of retinal layers, vitreoretinal interface, and choroid. OCT is based on low coherence interferometry wherein the backscattered light is measured to provide a high resolution (up to 1 µm) of the posterior pole. Imaging is performedin situand in real-time.
The OCT findings in CNVM indicate activity, location, type of CNVM based on the morphological characteristics. The various findings include subretinal (SRF), intraretinal fluid (IRF), hyperreflective material, both subretinal or sub RPE which can be due to blood, fibrin, CNVM complex composed of choroidal vasculature and scar element too, pigment epithelial detachments, hyperreflective foci and several other changes indicative of the type of pathology.6,14
CNVMs can thus be classified into various types based on the location of the CNVM complex on an OCT scan. The plane of separation being the RPE, the CNVM can be located sub RPE, subretinal or intraretinal, or a combination of the above.
Type 1: Sub RPE in location. The CNVM is seen below the RPE with PEDs, SRF, and IRF. A corresponding FFA in Type 1 CNVMs reveals an occult leak.
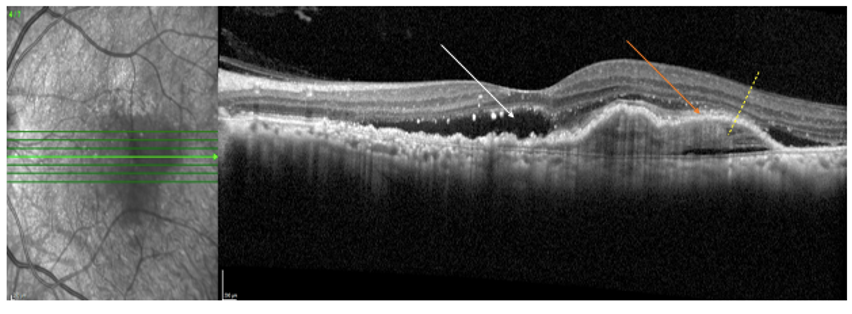
Figure 5A horizontal OCT raster scan passing through fovea showing Type 1 CNVM (sub-RPE CNVM) with SRF (white arrow), solid PEDs (orange arrow), and sub-RPE hyperreflectivity (yellow dashed arrow) suggestive of sub RPE blood/fibrin/CNVM complex all part of a typical Type 1 CNVM.
Type 2: Subretinal in location. The CNVM is seen as subretinal hyperreflective material with accompanying SRF or IRF. An FFA shows a lacy classic pattern of leak.
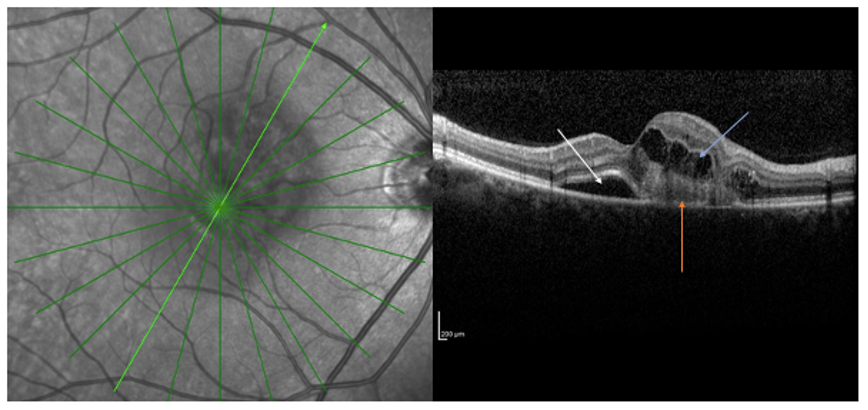
Figure 6A radial OCT scan of a Type 2 CNVM (subretinal CNVM) showing subretinal hyperreflective material (CNVM lesion- orange arrow) with subretinal fluid (white arrow) and intraretinal fluid (blue arrow).
Type 3: Retinal Angiomatous Proliferation (RAP) - Intraretinal in location with localised intraretinal hemorrhage on examination with intraretinal fluid and exudation on OCT. These cases are difficult to treat.
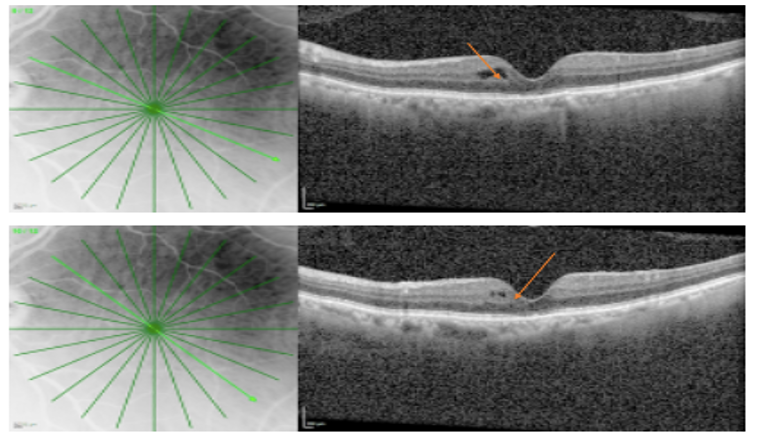
Figure 7OCT radial scan of a Stage 1 RAP lesion showing intraretinal hypo reflective/cystoid spaces with minimal intraretinal hyperreflectivity and disruption of inner and middle retinal layers.
Scarred CNVM: The typical SDOCT biomarkers in a scarred CNVM include a Subretinal hyperreflective material (SRHRM), chronic cystic changes and outer retinal tubulation (ORT) suggestive of degenerating photoreceptors and irreversible vision loss.
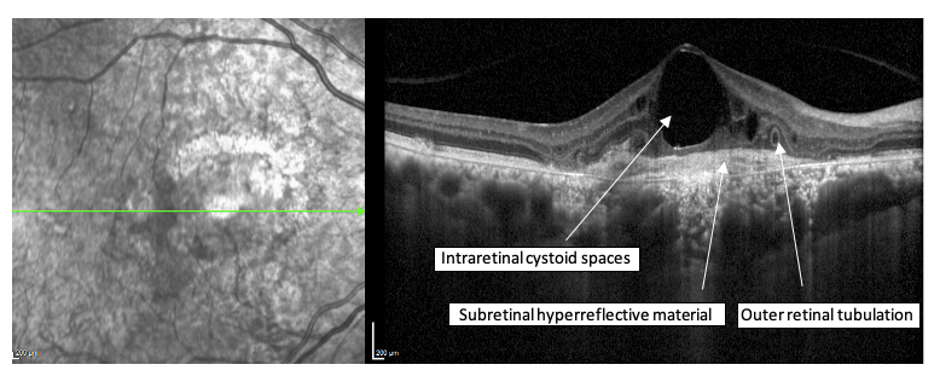
Figure 8A OCT line scan of a Scarred CNVM showing significant hyperreflective material, large cystic spaces with tubular hyperreflectivity (outer retinal tubules-ORT) in the outer retina indicative of chronicity. This presentation is associated with poor visual acuity due to extensive scarring and irreversible changes not amenable to treatment.
A typical CNVM regression pattern on SDOCT
A progressive decrease in Subretinal hyperreflective material can be seen with multiple anti-VEGF injections. The PEDs also decrease in the height and finally form a hyperreflective RPE clump/scar with minimal Subretinal fluid which warrants continuation of anti-VEGF therapy.
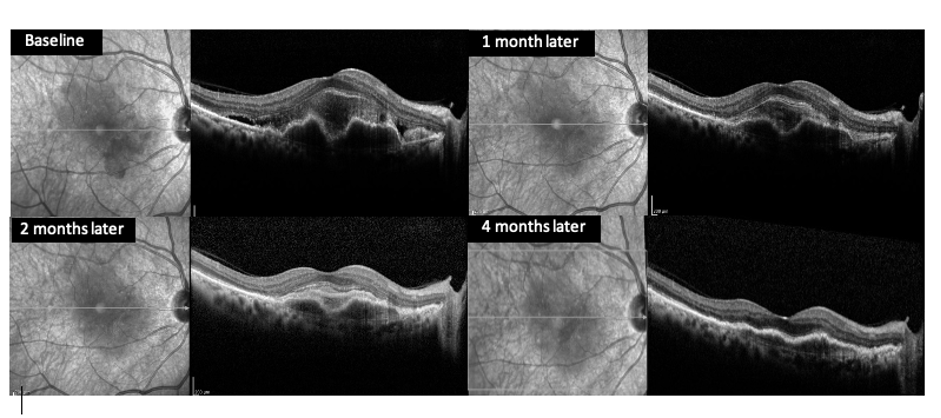
Figure 9A typical OCT-based documentation of regressing CNVM with treatment. The PED (orange arrows) and subretinal hyperreflective material (blue arrows) can be seen resolving with monthly intravitreal anti-VEGF injections.
Fundus fluorescein angiography (FA):
Fluorescein angiography is a diagnostic technique that allows the sequential visualization of blood flow simultaneously through retinal, choroidal, and iris tissues as the fluorescein dye is injected into the bloodstream via the vein in the arm. FA is based on the principle of fluorescence. Fluorescence is the luminescence that is maintained only by continuous excitation i.e. excitation at one wavelength occurs and is emitted immediately through a longer wavelength. The dye absorbs light in theblue rangeof the visible spectrum peaking at 465-490nm and emits light of the yellow-greenrange of visible spectrum peaking at 520-530nm. It determines the location, extent and boundaries, definition of CNVM, and its relation to the center of the fovea. FA highlights the retinal circulation and is of prognostic importance, in treatment and follow-up.23
Depending on the location of the leak in relation to the fovea, a typical FA can have a
Subfoveal: Under the fovea
Juxta foveal: Leak < 200 microns from the center of the fovea
Extra foveal: Leak > 200 microns from the center of the fovea
Based on the pattern of leak, the FA is classified as Classic and Occult leak.
A Classic leak has an early lacy pattern of hyper fluorescence with clear well-demarcated margins identified in the early phases of angiogram followed by mid and late phase leakage and pooling.23,24
An Occult CNVM on the other hand is classified into 2 types of leakage, a fibrovascular PED showing stippled hyper fluorescence with associated leakage and pooling showing up in the first 1 to 2 minutes of FA. The second leakage is the Late Leakage of Unknown Source (LLUS) seen as speckled hyper fluorescence with no clear boundaries of the lesion.24 The boundaries of these lesions on FA can be well defined or poorly defined, can be classified as predominantly CNV, predominantly classic CNV, predominantly CNV with a minimally classic composition, predominantly CNV with occult with no classic composition, predominantly hemorrhagic based on composition.24 A mixed lesion can also be seen.
Classic leak
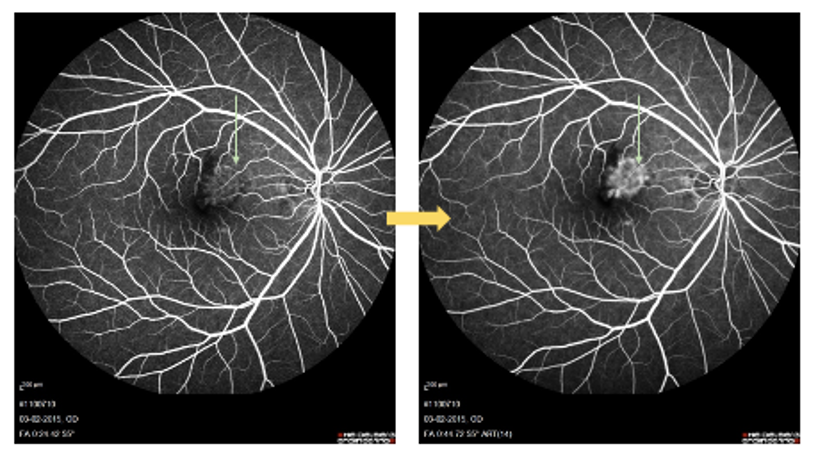
Figure 10FA of a Classic CNVM showing a well-defined, lacy pattern of leakage Increasing in intensity in later phases (green arrows). The Classic pattern of leakage corresponds to Type 2 or a Sub retinal CNVM.
Occult leak
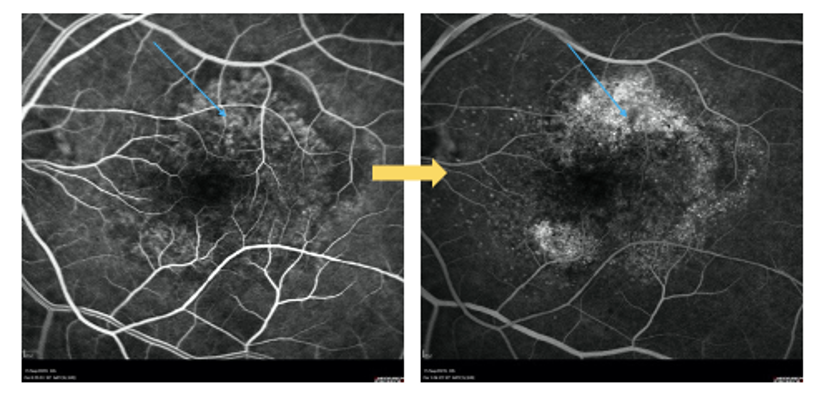
Figure 11FA of an Occult CNVM showing no particular area of leakage but areas of stippledhyper fluorescence (blue arrows) increasing in intensity in later phases. This pattern of leakage corresponds to Type 1 or Sub RPE CNVM.
Late Leakage from Unknown Source (LLUS)
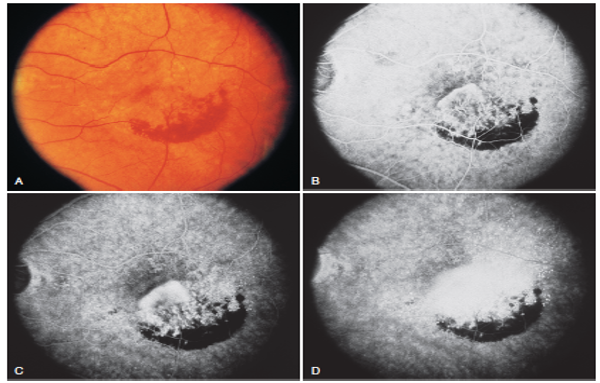
Figure 12A case of classic with an occult leak on FFA in early and mid-phases of FFA. Late phase shows leakage from an unidentified source not related to the prior leak. Source: Ryan Retina 6th edition. Original Images: Macular Photocoagulation Study GroupArch Ophthalmol 1991; 109:1242–57
Indocyanine green angiography (ICGA)
The ICG molecule has biophysical properties that make it useful for visualizing the choroidal circulation. The dye is excited by light close to infrared, increasing its penetration through the retinal pigment epithelium (RPE), melanin, xanthophyll pigment and thin blood layers. ICG circulates almost entirely bound to plasma proteins, and gradually diffuses across the choriocapillaris – thus allowing better visualization of its circulation within the choroidal vessels. These properties make it possible to visualize CNVM beneath blood layers, exudates or RPE detachments by differentiating between the hypo fluorescent serous component and the hyperfluorescent vascular component. Thus, it is more sensitive in detecting idiopathic polypoidal choroidal vasculopathy (IPCV) and choroidal circulation based lesions.
On ICGA, CNVM has been reclassified into three different morphologic types: focal spot or “hot spot”, plaques (well or poorly defined), and mixed (i.e., a combination of the previous two). These alterations may be located at the margin of the lesion (marginal spot), above the lesion (overlying spot), or at a distance from the lesion (remote spot).
ICGA is able to identify two elements in these anomalies: polypoidal structures projecting from the internal choroid towards the retina, and a branched choroidal vascular network (BVN) manifesting with early vascular hyper fluorescence.
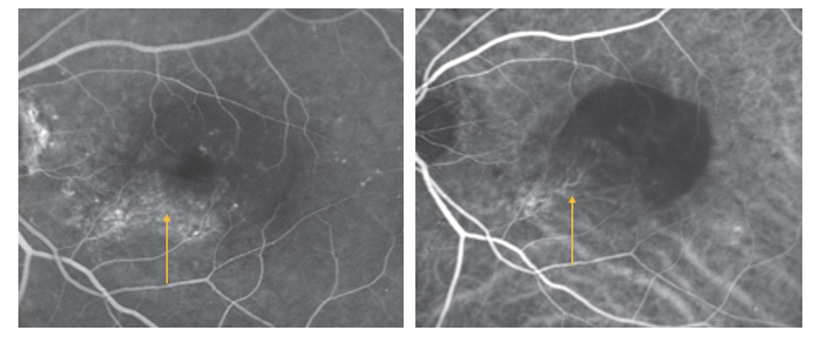
Figure 13FA image showing occult leak. A corresponding ICGA shows the choroidal vascular Network with a feeder vessel (yellow arrows).
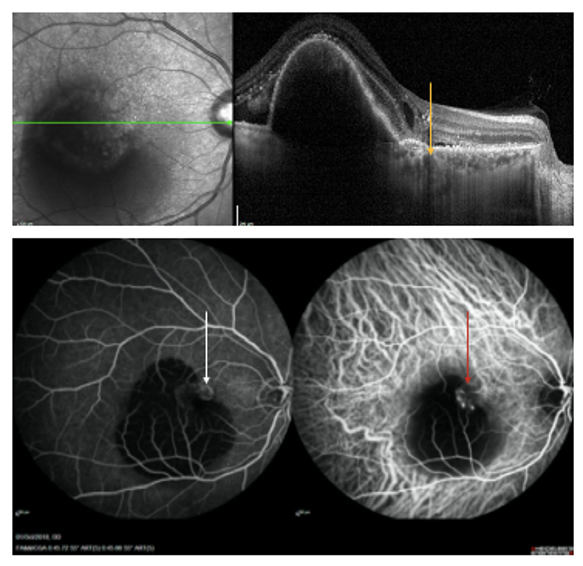
Figure 14A case of Idiopathic polypoidal choroidal vasculopathy (IPCV) with Branching vascular network (BVN) evident as double-layer sign beside a large PED on OCT (yellow arrow). The corresponding area appears as an occult leak on FA (white arrow) butICGA reveals polyps with BVN (red arrow).
Optical coherence tomography angiography
OCTA is OCT and Enface based dye less, non-invasive visualization of retinal and choroidal vasculature gaining popularity for its repeatability, safety, and obvious advantages but with its own set of limitations. OCTA has found a keen interest group in researchers and for exploratory purposes to understand the pathology and changes with treatment with several papers being published in recent years. The salient points in visualization of CNVM with OCTA include its ability to detect the CNVM vasculature, serial monitoring with response to treatment strategies and characterization of vasculature based on activity. The major disadvantages include compromised quality images in poor vision, imaging, and interpretation difficulties with artifacts in presence of fluid, blood, large RPE detachments, exudates, and media opacities.
OCTA is an evolving field with newer hardware and software innovations and image processing modalities over time thus enabling a better understanding of the pathology.
An OCTA image in comparison with FA. The mid phase of FA showing a classic leak and OCTA demonstrates the vascular network in great detail. (Figure 15)
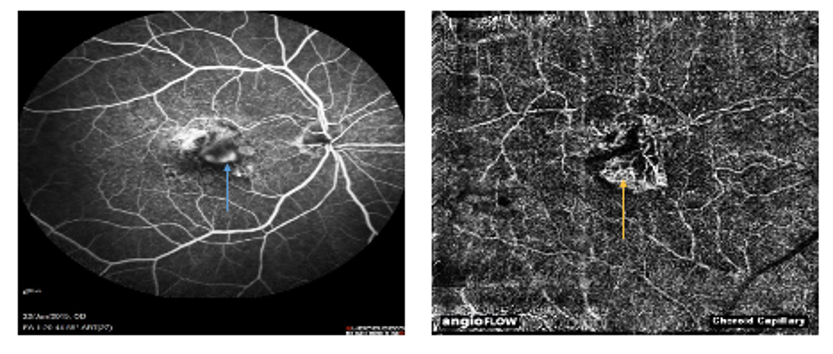
Figure 15FA showing classic leak with increasing hyper fluorescence obscuring the finer details of a CNVM complex (blue arrow). A chorio-capillary slab of OCT angiographyshows an extremely clear vascular complex corresponding to the leak on FA.
OCTA can also be used for monitoring the treatment response as evidenced by the shrinkage of the CNVM complex 4 weeks after anti-VEGF injection.
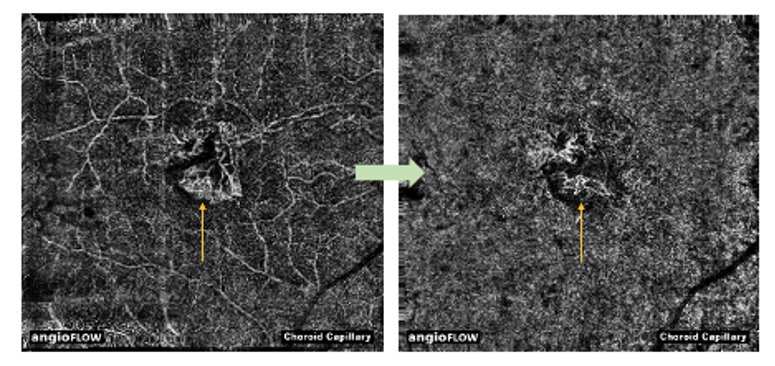
Figure 16A serial monitoring of CNVM complex with OCTA showing shrinkage of the CNVM complex 4 weeks after anti-VEGF injection (yellow arrows).
OCTA can also be used to quantify the vascularity and area of CNVM complex with inbuilt tools like Anglo analytics software of Optovue machine that is discussed here.
Serial measurement of the CNVM complex can thus be obtained.
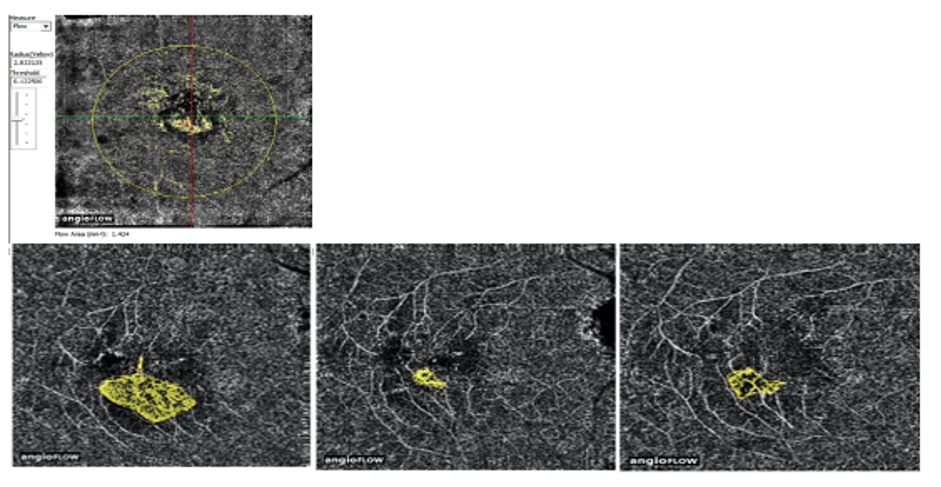
Figure 17A serial follow-up of CNVM on OCTA with the inbuilt software, Angio analytics on Optovue demonstrating the area and vascularity of the CNVM complex as aquantitative value.
Differential diagnosis of a CNVM
- Polypoidal choroidal vasculopathy (PCV)
- Central serous chorioretinopathy (CSCR)
- Choroidal tumours
The above conditions can be differentiated based on the age of presentation, laterality, associated features like drusens, PEDs, PCV, and choroidal lesional characteristic signs on OCT and clinical examinations. An FFA, ICGA, and ultrasonography wherever required would clinch the diagnosis.
Treatment modalities
Pharmacotherapy in the form of Anti VEGF agents is the mainstay of treatment for Neovascular AMD/CNVM. Before the advent of anti-VEGF treatment, Macular Photocoagulation Study (MPS) group (recruitment between 1981-1987) had treated CNVM with Krypton Laser photocoagulation. The results of the MPS study group recommended Krypton laser treatment for juxta foveal choroidal neovascular lesions with classic components but with a risk of recurrence. Mixed CNVMs with classic and occult CNVM did not benefit much from laser photocoagulation. The laser treatment extended at least 100 microns beyond the peripheral boundaries of the lesion. In subfoveal recurrent CNV, laser was performed at least 300 microns into the previous treatment scar and cover any feeder vessels with a uniformly white laser burn. 23
In 2001, the utility of Photo Dynamic Therapy (PDT) in CNVM was known which was developed in 1990s. PDT involves the use of an intravenous photosensitizing drug, Verteporfin, and a low-intensity non-thermal laser light of 689nm to cause a photochemical reaction and damage of choroidal neovascular tissue by direct cellular injury, damage to vascular endothelial cells, and vessel thrombosis.
TAP study group in 2001 showed that PDT can reduce the risk of moderate and severe visual acuity loss for at least 2 years in patients with predominantly classic subfoveal lesions.25 VIP trial in 2003, showed that PDT could reduce the risk of moderate and severe visual acuity loss at 2 years for occult with no classic component. 26
The present treatment is in the form of intravitreous injections. These include various Anti-Vascular Endothelial Growth Factor (anti-VEGF) agents. Various anti-VEGF agents include Bevacizumab (AVASTIN), a humanized murine monoclonal antibody binding VEGF-A; Ranibizumab (LUCENTIS), a humanized murine monoclonal antibody fragment, also binding VEGF-A; and Aflibercept (EYLEA), inhibits VEGF-Aas well asPlacentalGrowthFactor (PlGF).Corticosteroid injections have also been used in chronicity and certain recurrent cases in view of their anti-inflammatory properties.
Pegaptanib sodium (MACUGEN), an aptamer specifically inhibiting the VEGF-A 165 isoform was the first anti-VEGF to be approved by USFDA but was later replaced by the other anti-VEGF agents over years.27, 28, 29
Based on a Cochrane systematic review of literature and conclusions of various clinical trials, an approach to the management of subfoveal CNVM29,30 is summarized below
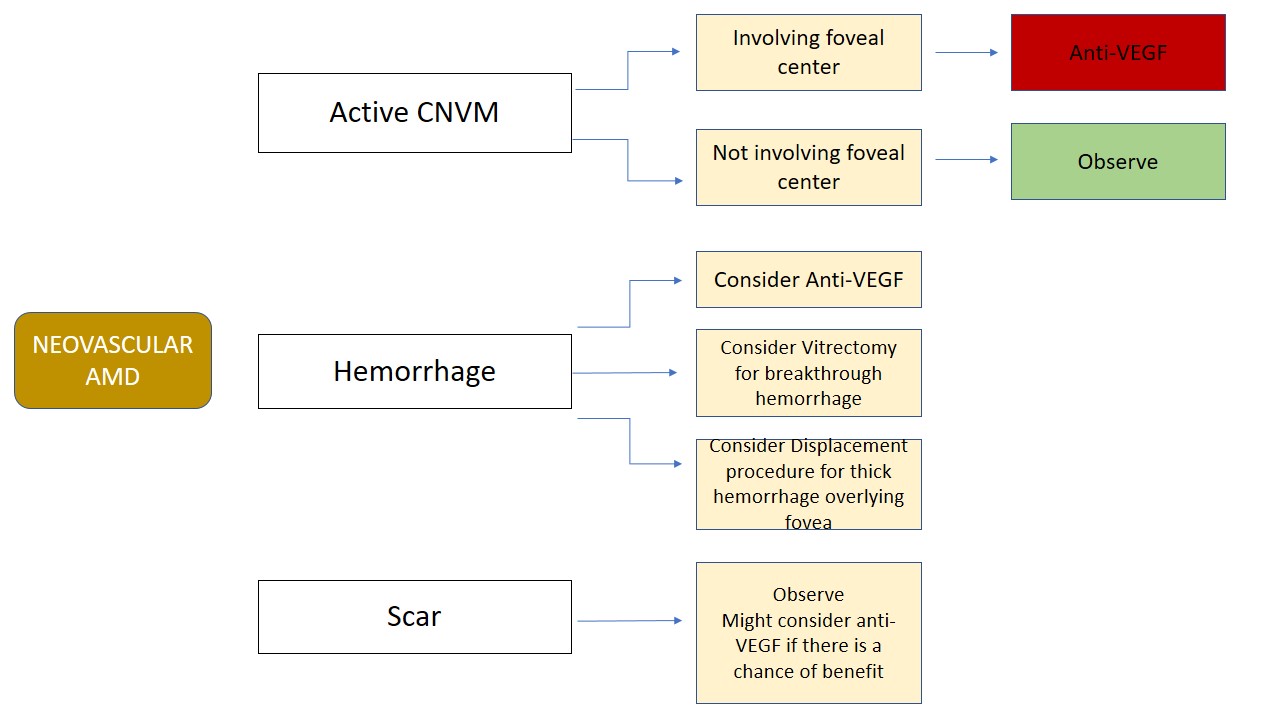
Table 4
The treatment and follow up regimen include
- Observe-and-plan regimen: Initial three loading doses, followed by a monthly observation
- PRN (pro re nata) strategy: individualized regimen based on monthly evaluation visits
- Treat-and-extend regimen: progressive lengthening of the intervals between the visit-injection dates
- Fixed regimen: monthly or bimonthly injections
There are several landmark clinical trials in CNVM that include anti-VEGF treatment alone and in combination with PDT. The important trials are summarized below
|
STUDY |
DRUG |
CONCLUSIONS |
|
MARINA |
RANIBIZUMAB |
2 years Ranibizumab prevented vision loss and improved mean VA, in minimally classic or occult (with no classic lesions) Most important predictors of VA outcomes were baseline VA , CNV lesion size and age |
|
ANCHOR |
RANIBIZUMAB |
Ranibizumab had greater clinical benefit than verteporfin PDT in new-onset, predominantly classic CNV |
|
HORIZON |
RANIBIZUMAB |
Multiple ranibizumab injections were well tolerated for 4 years. With Less frequent follow-up and treatment, there was an incremental decline in the VA gains achieved with monthly treatment |
|
CATT |
RANIBIZUMAB BEVACIZUMAB |
Both had similar effects on VA over a 2-year period Treatment as needed resulted in less gain in VA No differences in-between drugs in rates of death or arteriothrombotic event |
|
VIEW I/VIEW II |
AFLIBERCEPT RANIBIZUMAB |
Visual improvement achieved at week 52 was largely maintained through week 96 with both The original 2q8 aflibercept group achieved efficacy results that were similar to ranibizumab, with an average of 5.3 fewer injections over the 96-week period Intravitreal aflibercept had generally favourable safety through week 96 |
|
SEVEN-UP |
RANIBIZUMAB |
Approximately 7 years after ranibizumab therapy in the ANCHOR or MARINA trials, one-third of patients demonstrated good visual outcomes, whereas another one-third had poor outcomes Compared with baseline, almost half of eyes were stable, whereas one-third declined by 15 letters. even at this late stage in the therapeutic course, exudative AMD patients remain at risk for substantial visual decline |
Table 5Abbreviations: VEGF, vascular endothelial growth factor; AMD, age-related macular degeneration; VA, visual acuity; CNV, choroidal neovascularization; PDT, photodynamic therapy. Source: Al-Zamil WM, Yassin SA. Recent developments in age-related macular degeneration: a review.Clin Interv Aging. 2017;12:1313-1330. Published 2017 Aug 22. doi:10.2147/CIA.S143508
CATT trial second-year conclusions: (Source: Ryan Retina 6th edition)
The second year of the CATT was not designed to determine the relative efficacy of each dosing regimen for each medication. However, the following conclusions may be drawn:
1. In contrast to the first-year results, longer-term follow-up suggests that as-needed therapy is less effective than monthly therapy overall in terms of visual gain.
2. Visual acuity and visual gain are associated with but do not closely mirror, retinal thickness or presence of fluid.
3. One year of monthly therapy does not appear to confer lesion stability when subsequently changing to as-needed therapy.
4. When given as needed, bevacizumab is required more frequently than ranibizumab, on an average of 1.5 more injections over the 2-year period.
5. Geographic atrophy appears to occur with greater frequency in patients receiving monthly therapy.
6. SDOCT does not appear to increase the accuracy of identifying retinal fluid by the treating physician.
7. Endophthalmitis occurs at similar rates in ranibizumab and bevacizumab-treated patients, although (as one may expect) it appears to be associated with an increased rate of injections, occurring most often in patients treated monthly.
8. The increased rate of systemic serious adverse events in bevacizumab persisted in the second year. The authors remained unsure of the reason for the increased risk ratio of systemic adverse events.
The two-year CATT results certainly supported the continued off-label use of bevacizumab for exudative AMD. In addition, it appears that monthly dosing for any anti-VEGF therapy results in better and more sustained visual outcomes than as-needed dosing.
Radiation therapy
The rationale for radiation therapy is the fact that a CNVM is a proliferating neovascular tissue. External beam, plaques, or use of a probe with local irradiation have been used.31 A Cochrane systematic review concluded that there is not enough evidence to support this approach. A recent randomized controlled trial comparing epiretinal macular brachytherapy in 494 treatment-naive patients demonstrated that the radiation plus ranibizumab was inferior to quarterly or “as needed” ranibizumab.32, 33
Surgery
Several studies and a Cochrane systematic review reveal a poorer visual outcome following surgical interventions for CNVM. Sub macular surgery outcomes are no different compared to observation for subfoveal CNVM.34 The surgical techniques considered are macular translocation, displacement of large subretinal bleed with gas injection, and RPE transplantation. A macular translocation surgery is thus recommended only in patients with bilateral pathology and poor response to anti-VEGF agents. However, a media clearing vitrectomy can be considered in cases of vitreous hemorrhage secondary to a CNVM.
Risk of ‘other’ eye involvement
The MPS group revealed an incidence of 35% over 3 to 5 years of follow up. The risk factors include the presence of five or more drusen, one or more large drusen, focal hyperpigmentation, and systemic hypertension. An estimated 5-year incidence rate ranged from 7% for the subgroup with no risk factors to 87% for the subgroup with all four risk factors. Similarly, in AREDS, subjects enrolled with advanced AMD (either neovascular AMD or central atrophy of the RPE) in one eye only at study entry had a 43% chance of developing advanced AMD in the fellow eye by 5 years.22,35 These conclusions are important in the follow-up and counseling of patients with CNVM in one eye.
Future directions
Drugs in clinical trials for dry and wet AMD
|
Agents |
Targeted pathology |
Route of administration |
Mechanism of action |
|
Lampalizumab |
GA |
Intravitreal |
Anti-factor D Fab |
|
Oracea |
GA |
Oral |
Antibiotic-anti-inflammatory |
|
MTP- I3I(Ocuvia) |
GA |
Topical |
Mitochondrial protective compound |
|
MA09-hRPE |
GA |
Subretinal injection |
Human umbilical tissue-derived cells |
|
Brimonidine tartrate implant |
GA |
Intravitreal implant |
Alpha-2-antagonist |
|
Eculizumab |
GA |
Intravitreal |
mAb against complement factor CS |
|
E10030 |
Neovascular AMD |
Intravitreal |
Anti-PDGF PEGylated aptamer |
|
Proton radiation |
Neovascular AMD |
External radiation |
Radiation: proton radiation |
|
Abicipar pegol |
Neovascular AMD |
Intravitreal injection |
Anti-VEGF |
|
RTH258 |
Neovascular AMD |
Intravitreal injection |
Anti-VEGF |
Table 6
The development of sustained drug delivery systems would help in overcoming issues with the shorter half-life of anti-VEGF agents.36,37,38 These include
- Encapsulated cell technology (Neurotech Lincoln, RI, USA) with an implant releases both anti-PDGF and anti-VEGF (NT-506) is currently in preclinical development
- Port delivery system: For Sight VISION4 (Menlo Park, CA, USA). A refillable port drug delivery system (PDS).
- MicroPump (Replenish, Inc., Pasadena, CA, USA) - designed to release medication from a refillable reservoir into the eye at a controlled rate.
- Adeno-Associated Viral Vector (AAV) Gene Transduction: Gene therapy via viral vector genetic transduction with targets including VEGFR-1 and PEDF.
Others – combination therapies
- Pegpleranib (PDGF Inhibitor; Fovista): Combination therapy with ranibizumab targeting both VEGF and PDGF thus arresting the vessel growth
- OHR-102/squalamine: A VEGF, PDGF, and basic fibroblast growth factor (bFGF) inhibitor
- X-82: A VEGF and PDGF receptor antagonist
- Zimura: complement factor inhibitor
Rehabilitation
All AMD patients need to be educated regarding prognosis, possible treatment strategies, and visual outcomes. A prompt referral to the Low Vision Aid center has to be considered as and when the need arises.
References
- Bressler NM, Bressler SB, Congdon NG, et al. Potential public health impact of Age-Related Eye Disease Study results: AREDS report no. 11. Arch Ophthalmol 2003; 121:1621–4
- Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014; 2:e106–16. [PubMed: 25104651]
- Ferris FL, Fine SL, Hyman L. Age-related macular degeneration and blindness due to neovascular maculopathy. Arch Ophthalmol 1984;102(11):1640–2.
- Lambert NG, El Shelmani H, Singh MK, et al. Risk factors and biomarkers of age-related macular degeneration.Prog Retin Eye Res. 2016;54:64-102. doi:10.1016/j.preteyeres.2016.04.003
- Black JR, Clark SJ. Age-related macular degeneration: genome-wide association studies to translation.Genet Med. 2016;18(4):283-289. doi:10.1038/gim.2015.70
- Al-Zamil WM, Yassin SA. Recent developments in age-related macular degeneration: a review.Clin Interv Aging. 2017;12:1313-1330. Published 2017 Aug 22. doi:10.2147/CIA.S143508
- Kijlstra A, Berendschot TT. Age-related macular degeneration: a complementopathy? Ophthalmic Res. 2015;54(2):64–73.
- Okubo A, Rosa RH Jr, Bunce CV, et al. The relationships of age changes in retinal pigment epithelium and Bruch’s membrane. Invest Ophthalmol Vis Sci. 1999;40(2):443–449.
- Feeney-Burns L, Burns RP, Gao C. Age-related changes in humans over 90 years old. Am] Ophthalmol. 1990; 109:265-278.
- Pauleikhoff D, Harper CA, Marshall J, et al. Aging changes in Bruch's membrane: a histological and morphologic study. Ophthalmology.1990;97:171-178.
- Green WR, McDonnell PJ, YeoJ H. Pathologic features of senile macular degeneration. Ophthalmology. 1985;92(5):615–627.
- Green WR, Enger C. Age-related macular degeneration histopathologic studies. The 1992 Lorenz E. Zimmerman Lecture.Ophthalmology 1993;100(10):1519–35.
- Killingsworth MC, Sarks JP, Sarks SH. Macrophages related to Bruch’s membrane in age-related macular degeneration. Eye (Lond) 1990;4(4 Pt 4):613–21.
- Ambati J, Ambati BK, Yoo SH, Ianchulev S, Adamis AP. Age related macular degeneration: etiology, pathogenesis, and therapeutic strategies. Surv Ophthalmol 2003;48(3):257–93.
- Friedlander M, Brooks PC, Shaffer RW, Kincaid CM, Varner JA, Cheresh DA. Definition of two angiogenic pathways by distinct alpha v integrins. Science 1995;270(5241):1500–2.
- Miller JW. Vascular endothelial growth factor and ocular neovascularization. Am J Pathol 1997;151(1):13–23.
- Ferrara N. Vascular endothelial growth factor: basic science and clinical progress. Endocr Rev 2004;25(4):581–611.
- Robinson CJ, Stringer SE. The splice variants of vascular endothelial growth factor (VEGF) and their receptors. J Cell Sci 2001; 114(Pt 5):853–65.
- Ferrara N. Vascular endothelial growth factor: basic science and clinical progress. Endocr Rev 2004;25(4):581–611.
- Ferris FL, Davis MD, Clemons TE, et al. A simplified severity scale for age-related macular degeneration: AREDS Report No. 18.Arch Ophthalmol. 2005;123(11):1570-1574. doi:10.1001/archopht.123.11.1570
- Bird AC, Bressler NM, Bressler SB, et al. An international classification and grading system for age-related maculopathy and age-related macular degeneration. The International ARM Epidemiological Study Group.Surv Ophthalmol.1995;39(5):367–374.
- AREDS-Study-Group A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8.Arch Ophthalmol.2001;119(10):1417–1436.
- Macular Photocoagulation Study Group. Subfoveal neovascular lesions in age-related macular degeneration. Guidelines for evaluation and treatment in the macular photocoagulation study. Arch Ophthalmol 1991;109(9):1242–57.
- Ryan 6th edition
- Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: two-year results of 2 randomized clinical trials – TAP report 2. Arch Ophthalmol 2001;119(2): 198–207
- Barbazetto I, Burdan A, Bressler NM, et al. Photodynamic therapy of subfoveal choroidal neovascularization with verteporfin: fluorescein angiographic guidelines for evaluation and treatment – TAP and VIP report no. 2. Arch Ophthalmol 2003;121(9):1253–68.
- Comparison of Age-related Macular Degeneration Treatments Trials Research Group. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology 2012;119(7):1388–98.
- The CATT Research Group. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med 2011;364(20):1897–908.
- Solomon SD, Lindsley K, Vedula SS, Krzystolik MG, Hawkins BS. Anti-vascular endothelial growth factor for neovascular age related macular degeneration. Cochrane Database Syst Rev 2014;(8):CD005139.
- Bressler NM. Antiangiogenic approaches to age-related macular degeneration today. Ophthalmology 2009;116(10 Suppl.):S15–23.
- A prospective, randomized, double-masked trial on radiation therapy for neovascular age-related macular degeneration (RAD Study). Radiation therapy for age-related macular degeneration. Ophthalmology 1999;106(12):2239–47.
- Evans JR, Sivagnanavel V, Chong V. Radiotherapy for neovascular age-related macular degeneration. Cochrane Database Syst Rev 2010;(5):CD004004.
- Jackson TL, Dugel PU, Bebchuk JD, et al. Epimacular brachytherapy for neovascular age-related macular degeneration (CABERNET): fluorescein angiography and optical coherence tomography. Ophthalmology. 2013;120(8):1597-1603.
- Eandi CM, Giansanti F, Virgili G. Macular translocation for neovascular age-related macular degeneration. Cochrane Database Syst Rev 2008;(4):CD006928.
- Macular Photocoagulation Study Group. Risk factors for choroidal neovascularization in the second eye of patients with juxtafoveal or subfoveal choroidal neovascularization secondary to age-related macular degeneration. Arch Ophthalmol 1997;115(6): 741–7
- Rivera ML, Lelis A, Bouchard B, et al. Pharmacokinetics of a VEGF antagonist delivered by an intraocular encapsulated cell technology implant. ARVO Annual Meeting Abstract; Ft. Lauderdale, FL. Invest Ophthalmol Vis Sci 2012;53:474.
- Guerrero-Naranjo JL, Quiroz-Mercado H, Sanchez-Bermudez G, et al. Safety of implantation of the NT-503 device in patients with Choroidal neovascularization secondary to age-related macular degeneration. Invest Ophthalmol Vis Sci 2013;54(15):3298.
- Kauper K, Rivera M, Mills J, et al. Design considerations and performance of a next-generation encapsulated cell technology intraocular implant delivering VEGF-antagonist. ARVO Meeting Abstract; Orlando, FL. Invest Ophthalmol Vis Sci 2014;55:441.