
Question
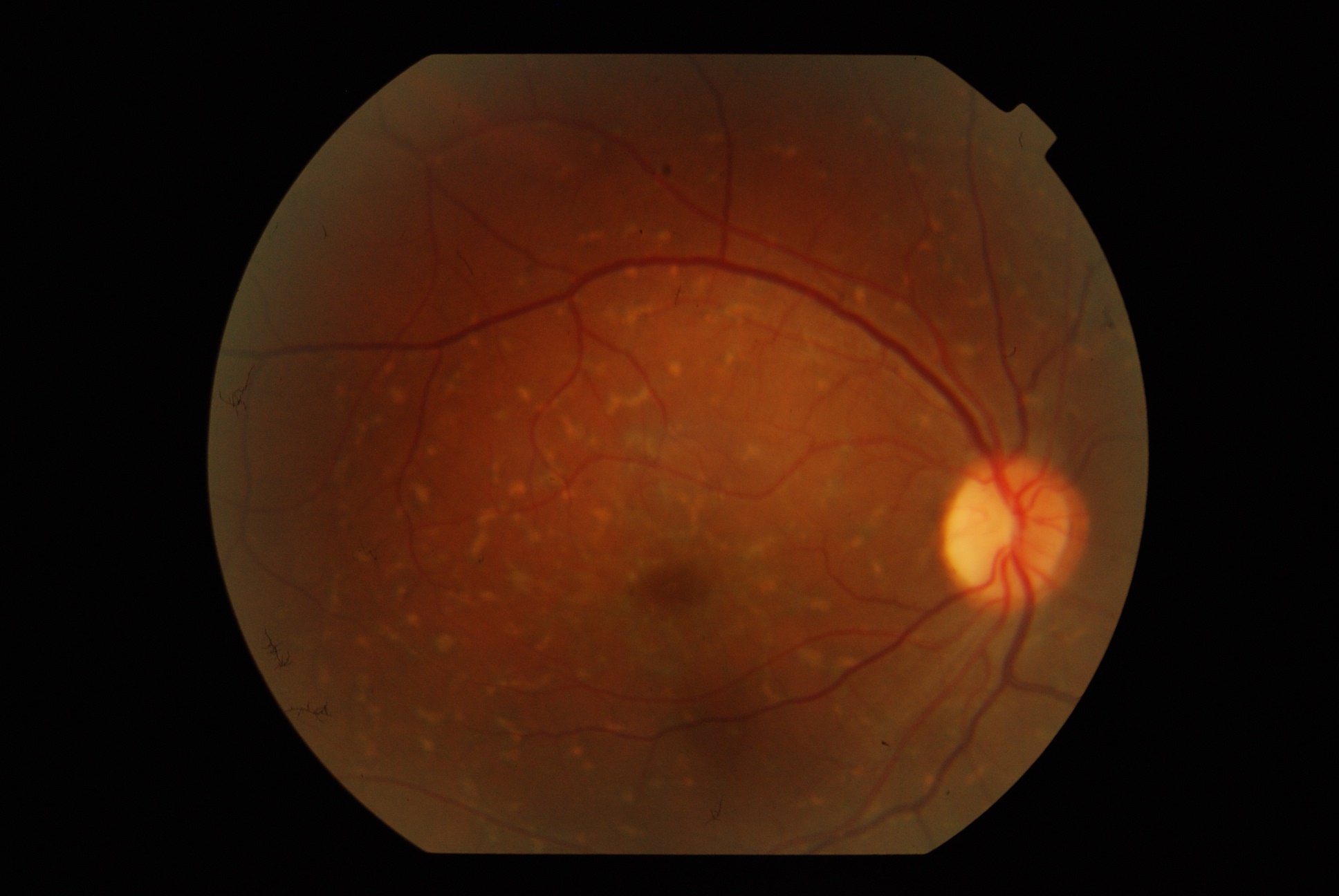
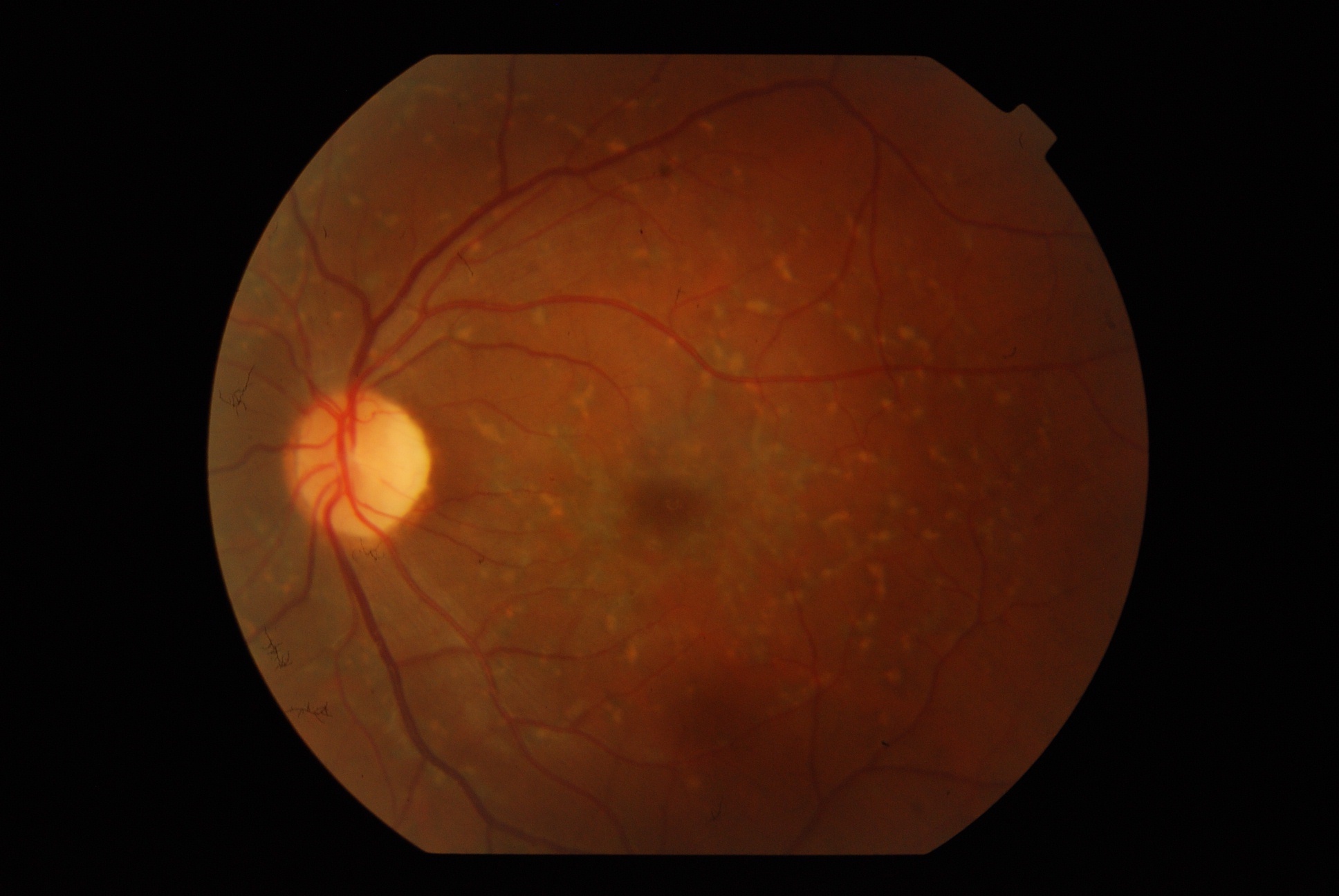
A 35-year-old otherwise healthy female ( computer professional) presented with OU diminution noticed recently. BCVA OD 6/12 N6 and OS 6/18 N8. Anterior segment including IOP were normal in both eyes. Fundus examination revealed as depicted in the color fundus photo.
-
What is the diagnosis( a differential is preferred)
-
How do you manage this case
Answer:
The diagnosis isStargardt’s Disease(SD)/Fundus flavimaculatus (FFM)
Few Features:
The onset of SD is generally in the first or second decade of life whereas FFM generally manifests after the 3 decades.
The main presenting symptoms generally decrease in central vision.VISUAL ACUITY DOES NOT CORRELATE WITH FUNDUS APPEARANCE.Dyschromatopsia, nyctalopia, and visual field loss are generally not present.
The earliest clinical sign is the loss of the foveolar reflex with symmetrical RPE alterations. Atrophy of fovea is generally marked by granularity, mottling, and presence of FLECKS(irregular-shaped yellow-white lesions with shapes ranging from round, linear, crescentic, or PISCIFORM). As the disease progresses the flecks increase in number and start becoming confluent and extend towards the equator.
The macula typically takes on a Tapetal reflex( Beaten Bronze appearance). In the course of the disease, the flecks gradually disappear and new flecks appear in a different location Disappearance of flecks is associated with RPE alterations and atrophy of the choriocapillaris. Subretinal pigmentary clumps may form, CNVM is a rare but a possible complication
The flecks can be confused with drusens to few, FFA is an excellent tool to differentiate
Drusens: often hyperfluoresce early and fade late
Flecks: do not fluoresce
Generally speaking, the diagnosis of SD/FFM is made clinically but few investigations are needed to rule out other mimicking conditions.
Fields: generally show a central scotoma
ERG: full-field ERG is generally normal and this helps in ruling out other conditions. However, mfERG may be abnormal
SD-OCT helps in studying the retinal layers which get damaged especially the PHOTORECEPTOR layers.
DARK CHOROID in FFA: It is an FFA diagnostic sign seen mainly in SD/FFM where the choroid appears dark secondary to absorption by the deposited LIPOFUSCHIN of the excitatory blue wavelength. The absence of dark choroid does not rule out SD/FFM but the presence of this feature is highly diagnostic.
There are few classifications of SD/FFM but have clinically very fewer implications. Names of few classification systems are
- NOBLE and CARR
- FISHMAN
- AABERG
Few terminologies
- PURE STARGARDT’S: Macular degeneration with perifoveal flecks
- PURE FFM: diffuse flecks without macular degeneration
The Differential Diagnoses are
- Fundus albipunctatus
- RP albescens
- Familial drusens
- Flecked retinal syndrome of Kandori
- Progressive cone dystrophy
- Vitelliform macular dystrophy
Cause of visual loss:
Mutation in ABCA4→ Affects the Rim protein which is a transporter in the rod outer segment →Accumulation of lipofuschin constituent( A2E) within RPE cells→Damage of photoreceptor cells
Managing these cases just involves a periodical retinal evaluation and monitoring any signs of a sudden decrease in vision that might indicate a developing CNVM( rare)