
What are prisms?
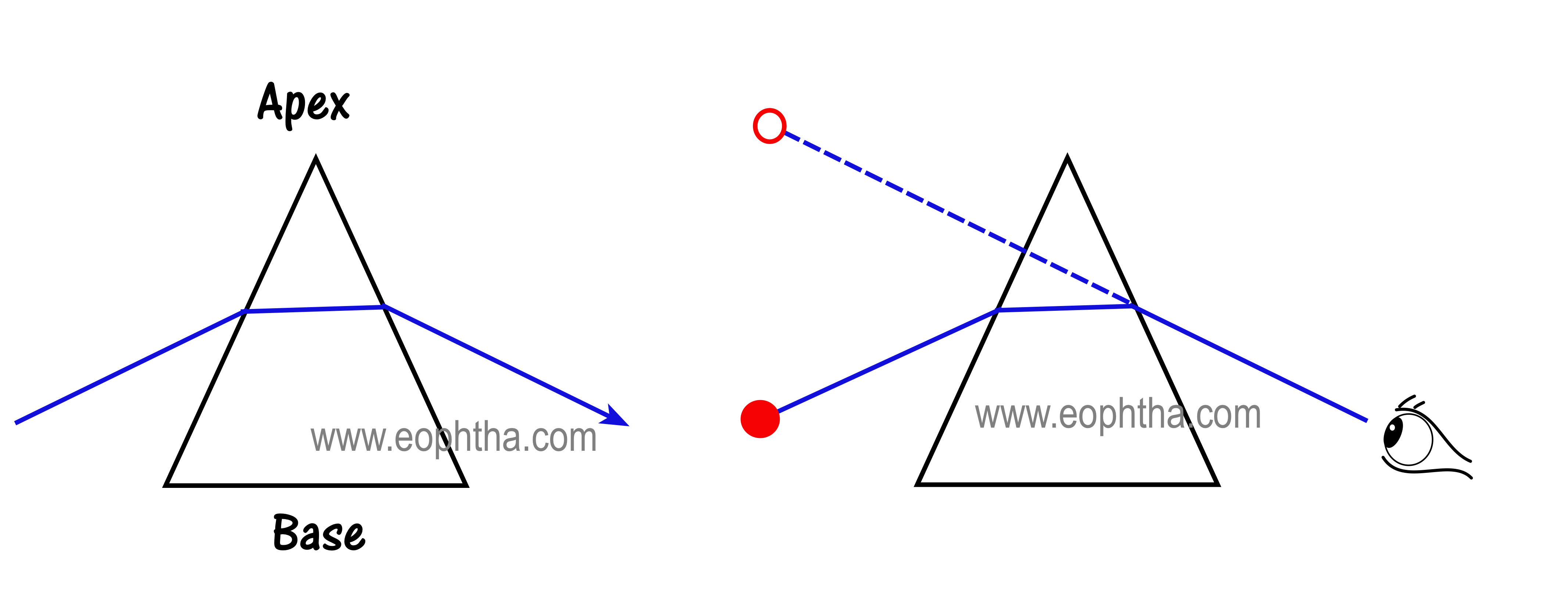
Prisms are nothing but a portion of a refracting medium bordered by two plane surfaces that are inclined at a finite angle. Prisms have a thicker portion called the base of the prism and a tapering portion called the apex of the prism. Prisms are oriented with their apex towards the direction of deviation.
What happens to light when it enters a prism?
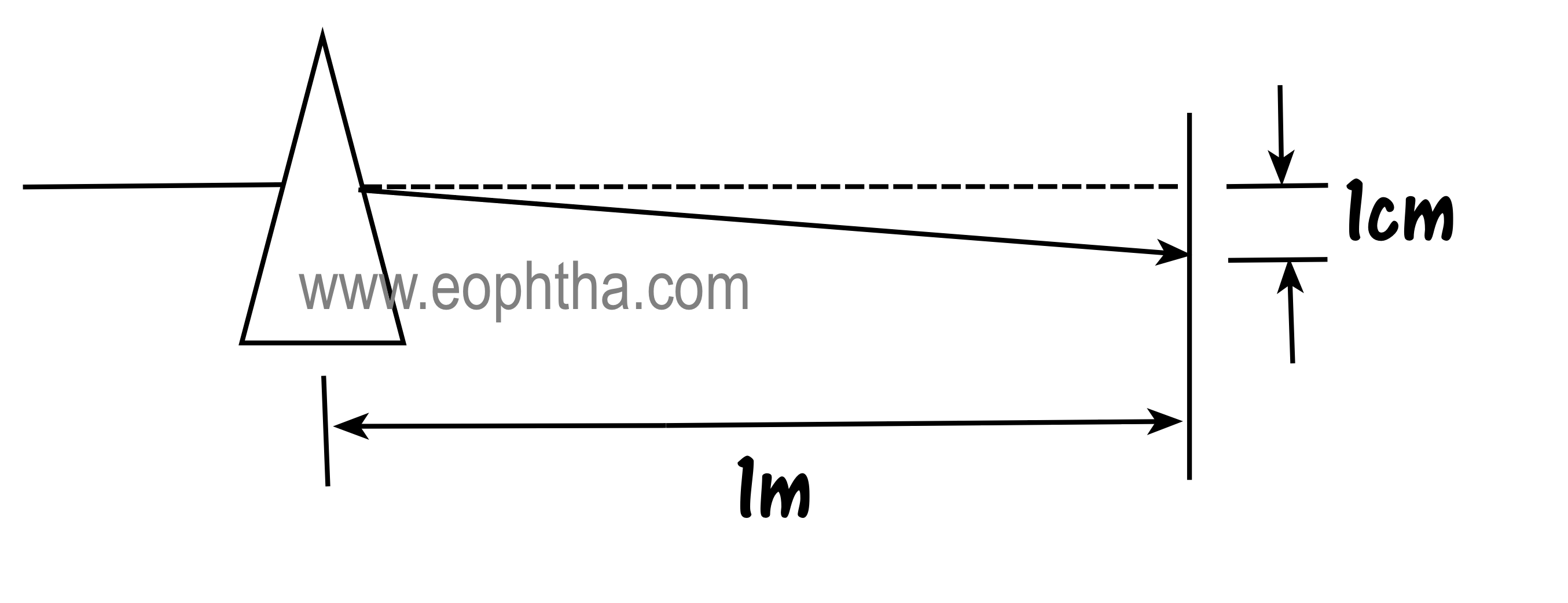
Light has particle and wave characteristics. When it travels through the thicker base of the prism, the particle form of light has to travel a longer distance than at the apex of the prism, this difference causes light to bend towards the base of the prism. The power of a prism to bend light is measured in prism diopters (PD). One prism diopter will shift light by 1 cm at 1m distance.
Calibration of Prism
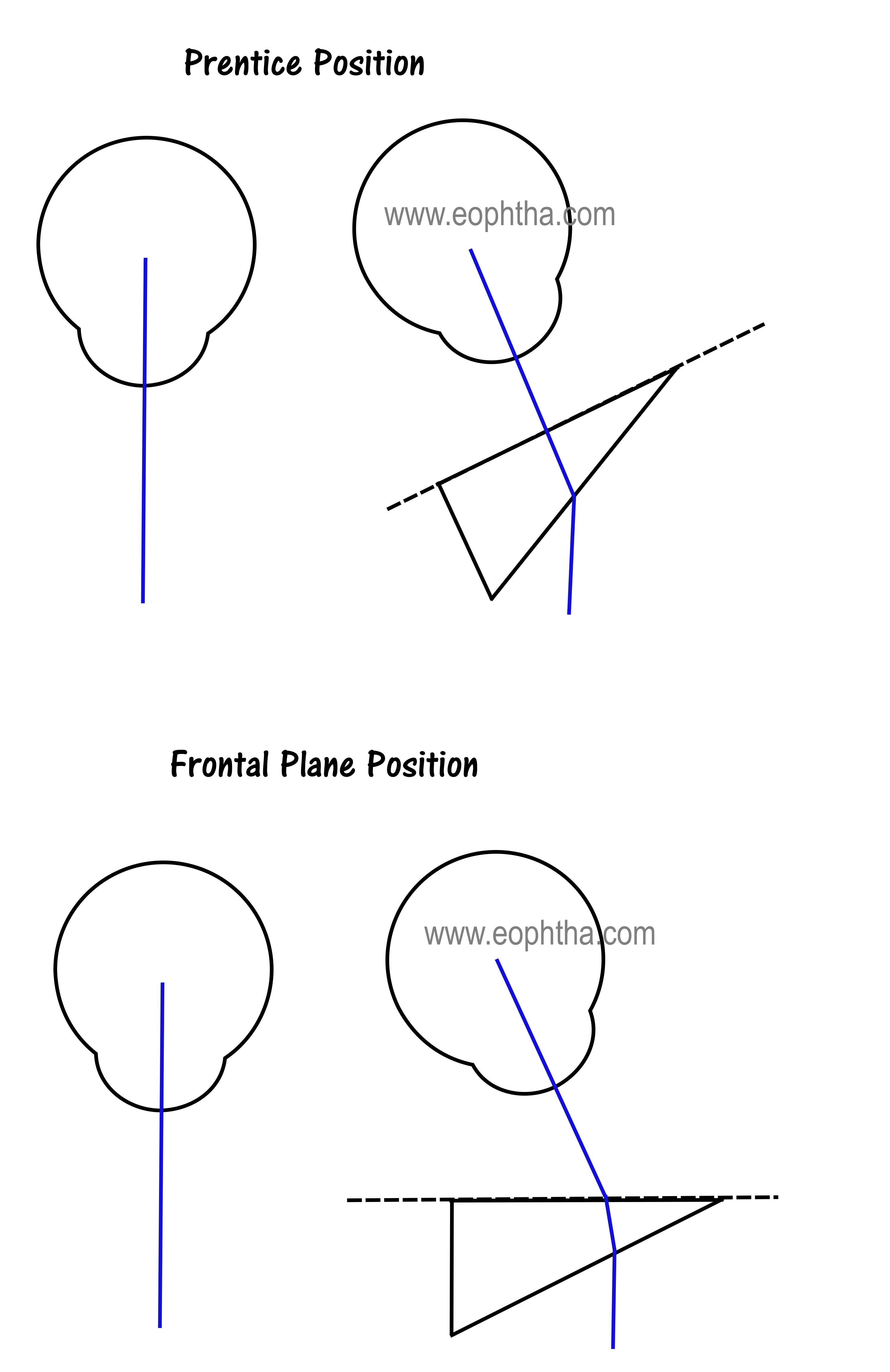
Prisms made of glass are calibrated in Prentice position. They should be held with the back surface perpendicular to the line of sight.
Plastic prisms and prism bars are calibrated by the angle of minimum deviation. They should be held with a back surface parallel to the face or in the frontal plane position.
The shift in Image with Prism
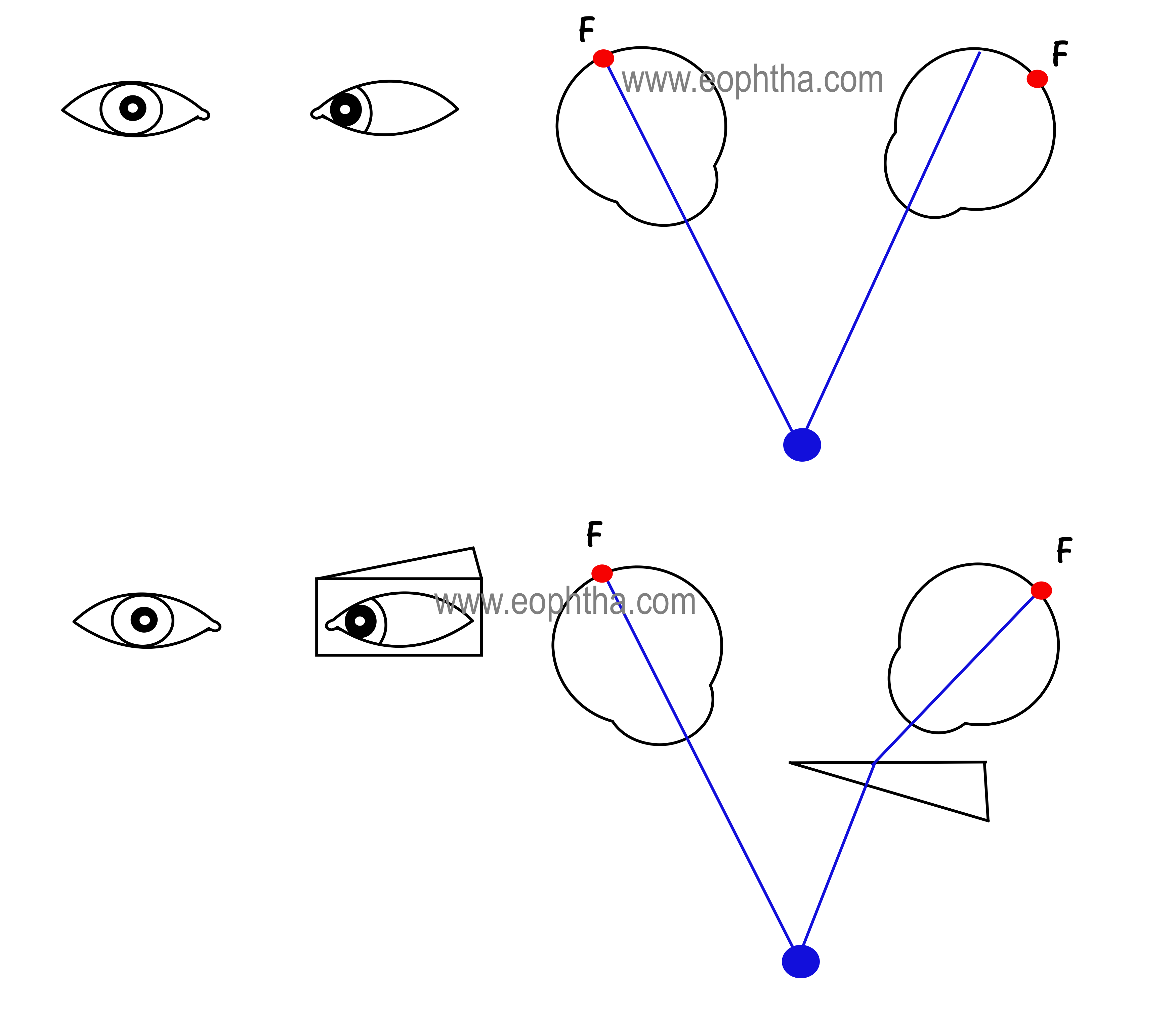
When a prism is placed in front of the eye, the retinal image is shifted towards the base of the prism. The perceived image moves towards the apex of the prism. This is the image jump which causes the eye to move in the direction of the apex of the prism to align the fovea with the new image location.
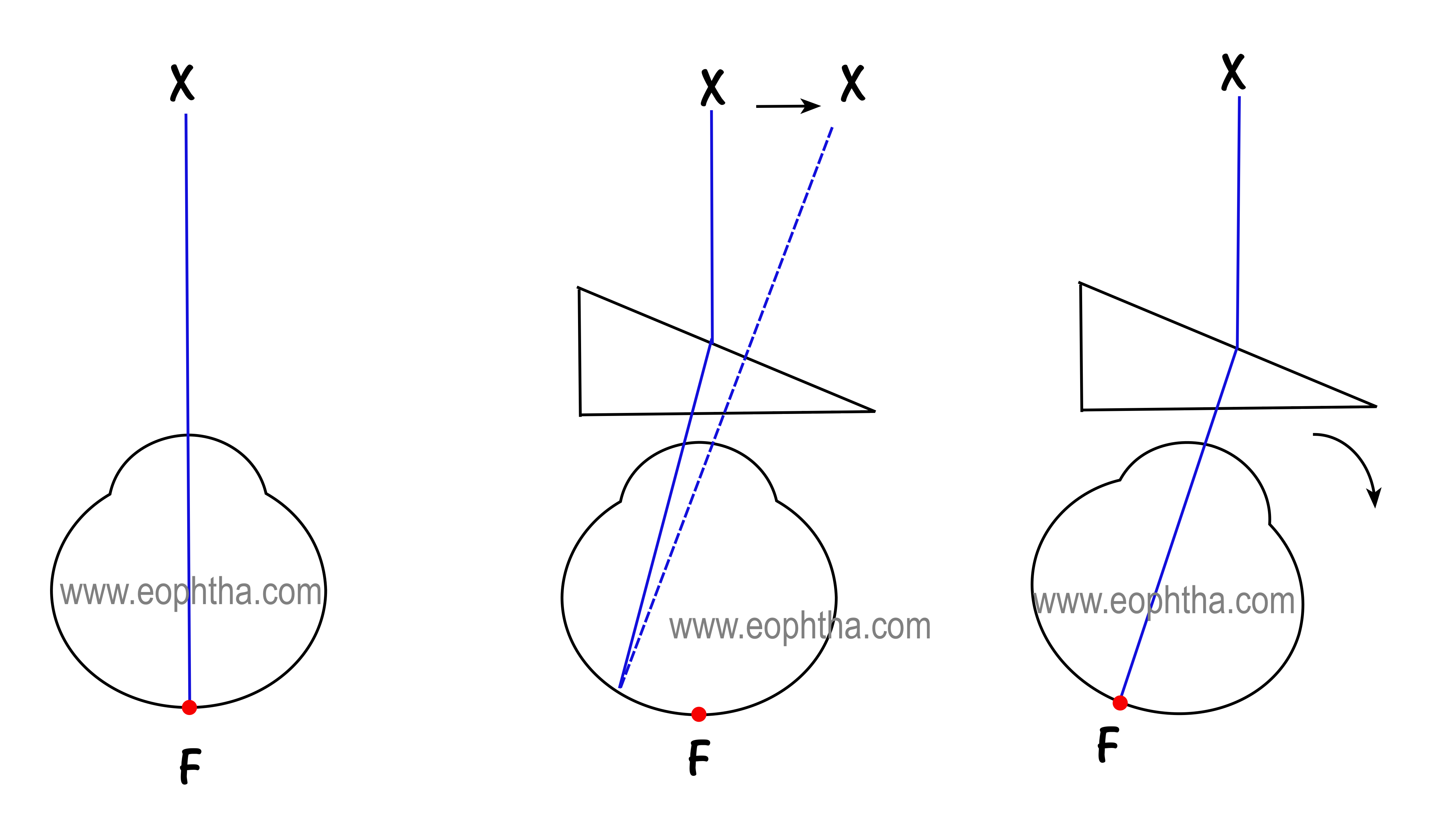
The firstpicture shows the patient fixing at object X
Second picture: A prism is introduced which displaces the retinal image off the fovea towards the base causing the perceived image to move towards the apex (image jump).
Third picture: This causes the eye to move or rotate towards the apex so that the retinal image falls on the fovea again. The refixation movement is always towards the apex of the prism.
There are three important concepts one needs to be well versed as regards to prisms:
- Neutralization of deviations with prisms
- Prism induced strabismus in orthotropia
- Prism induced vergence in orthotropia
How To Use Prisms To Measure Deviation:
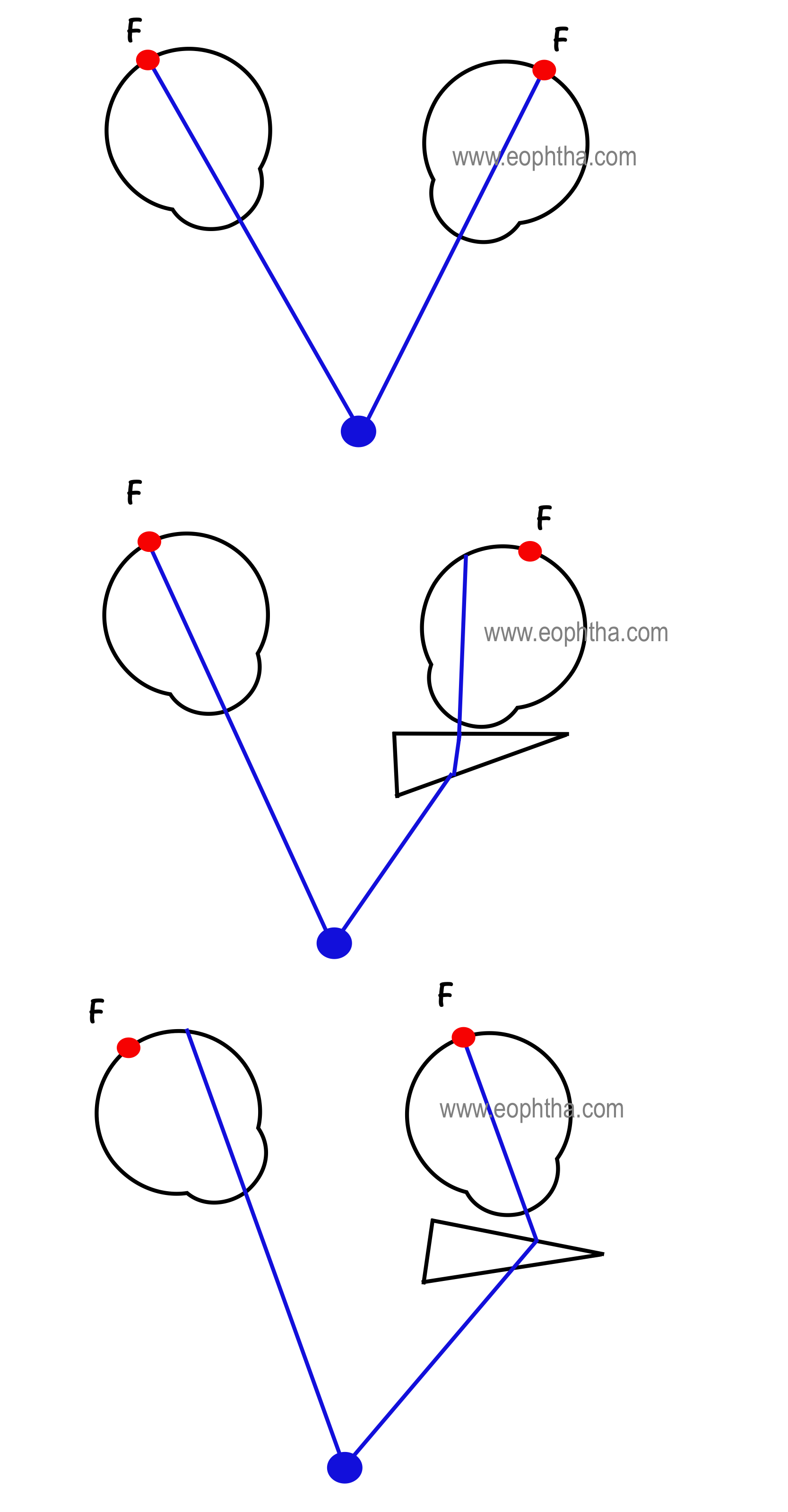
The rule for neutralizing a deviation is to place the prism with its apex oriented towards the direction of the deviation. An esotropia is neutralized with BASE OUT prisms. In esotropia, the image falls nasal to the fovea. Base out prism of appropriate strength will deflect the retinal image temporally on to the fovea as shown in the picture. Remember prisms can be placed in front of either eye to neutralize deviations. The strength of the prism needed to shift the image on to the fovea will neutralize the deviation and gives the measure of the deviation. BASE IN prisms neutralize exodeviations and BASE DOWN prisms neutralize hypertropia.
IMPORTANT CONCEPT: Always orient prisms with the apex in the direction of deviation.
Prism Induced Strabismus:
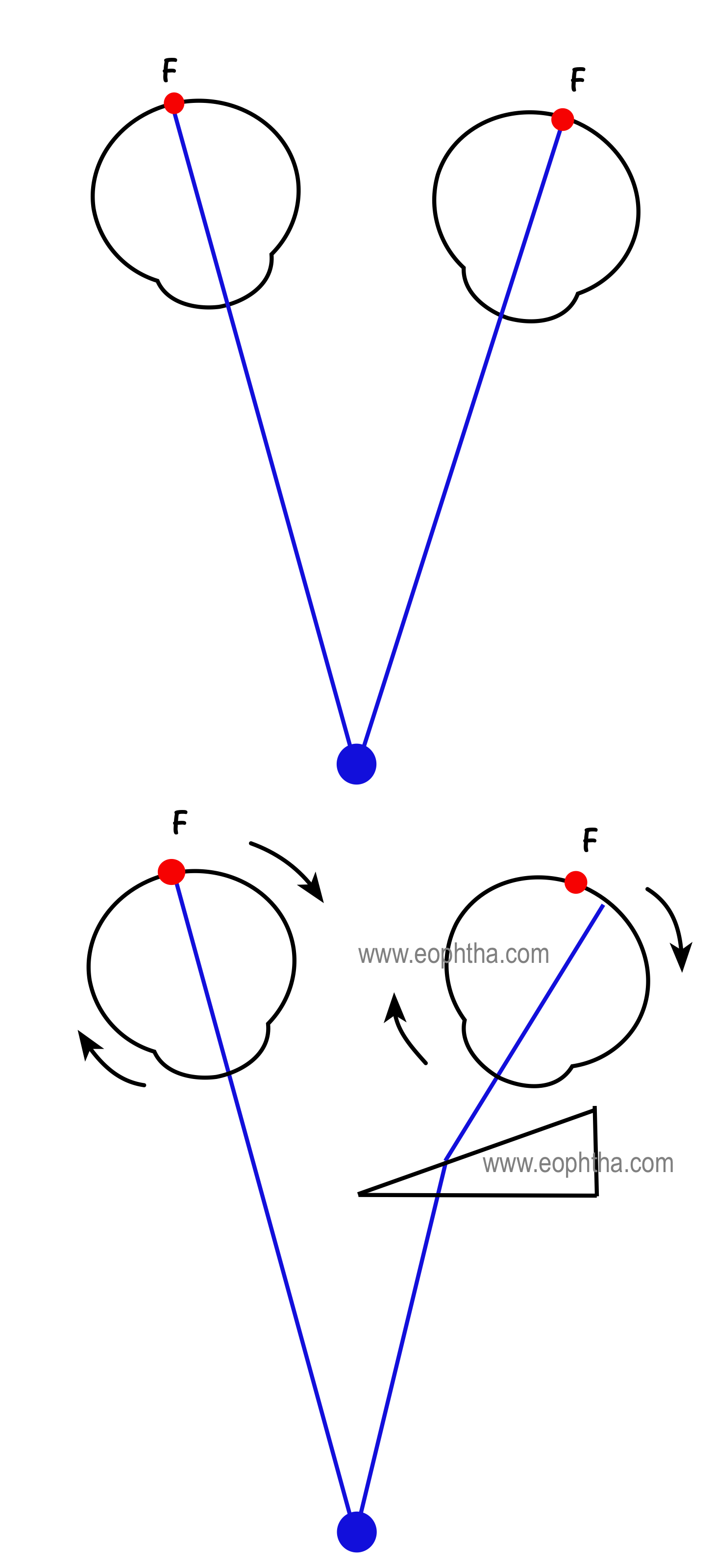
Patient with straight eyes (ORTHOTROPIA) and binocular vision is made esotropic by placing a base-in prism over one eye (in this case left eye). When a BASE IN prism is introduced the retinal image is displaced nasal to the fovea in the left eye. To place the image on the fovea the left eye moves temporally and therefore as per Herring’s law the right eye moves nasally and hence the retinal image is displaced nasally off the fovea in the right eye. Since base in prisms displaces retinal images nasal to the fovea, they produce optically induced esotropia. This is the basis for the induced tropia test used to detect suppression or amblyopia in certain cases. BASE OUT prisms produce optically induced exotropia.
Prism Induced Vergence:
When prisms induce optical esotropia as in BASE IN PRISMS they cause fusional divergence.
When prisms induce optical exotropia as in BASE OUT PRISMS, they cause fusional convergence,
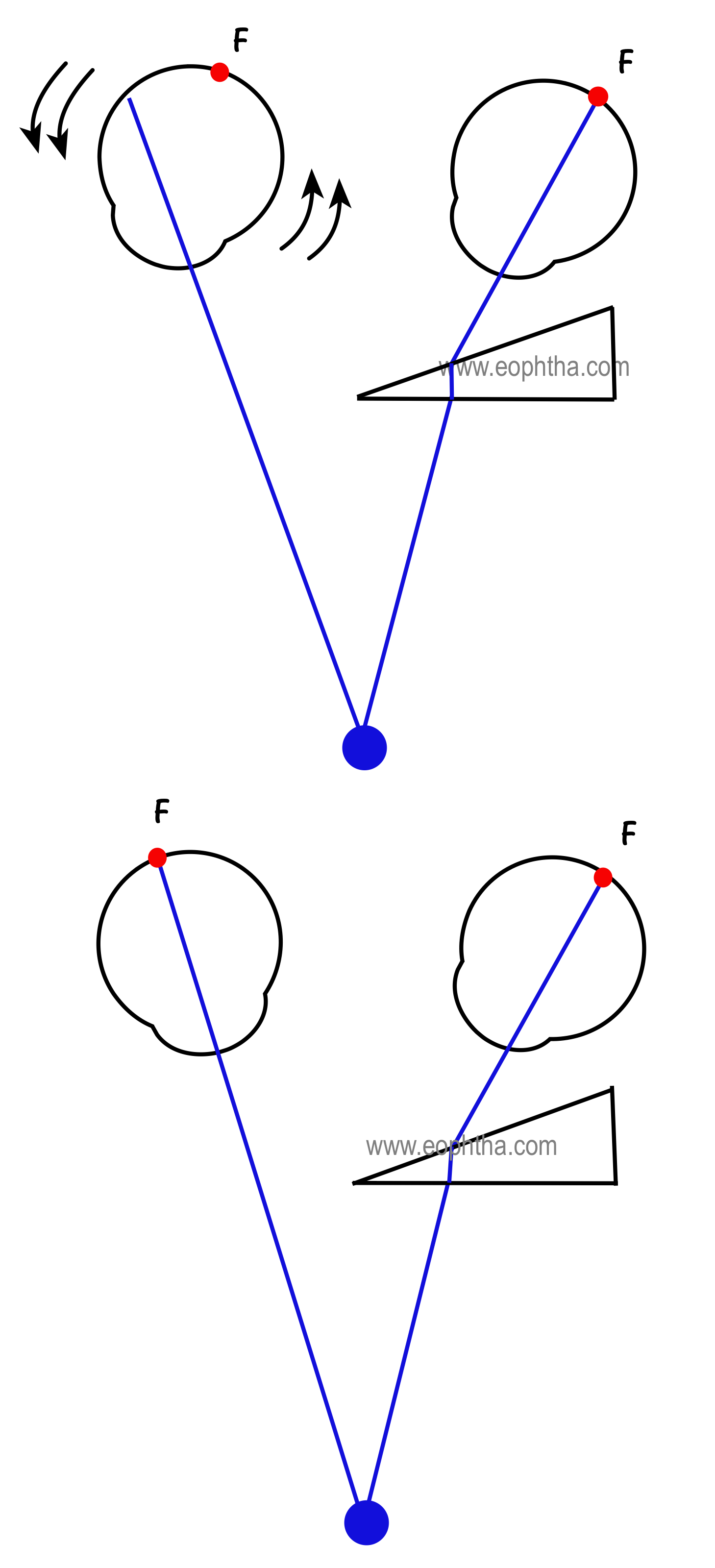
First Picture: orthotropic with bifoveal fusion
Second Picture: optically induced exotropia due to base out prism. The base out prism causes retinal image to be displaced temporal to the fovea. The left eye moves in and the right eye moves out as per Herring's law.
Third Picture: -This causes the image in the right eye to be displaced temporally off the fovea. So in order to fuse, the right eye makes inward or nasal movement producing fusional convergence. So base out prisms produces fusional convergence.
Fourth Picture: Fusion achieved
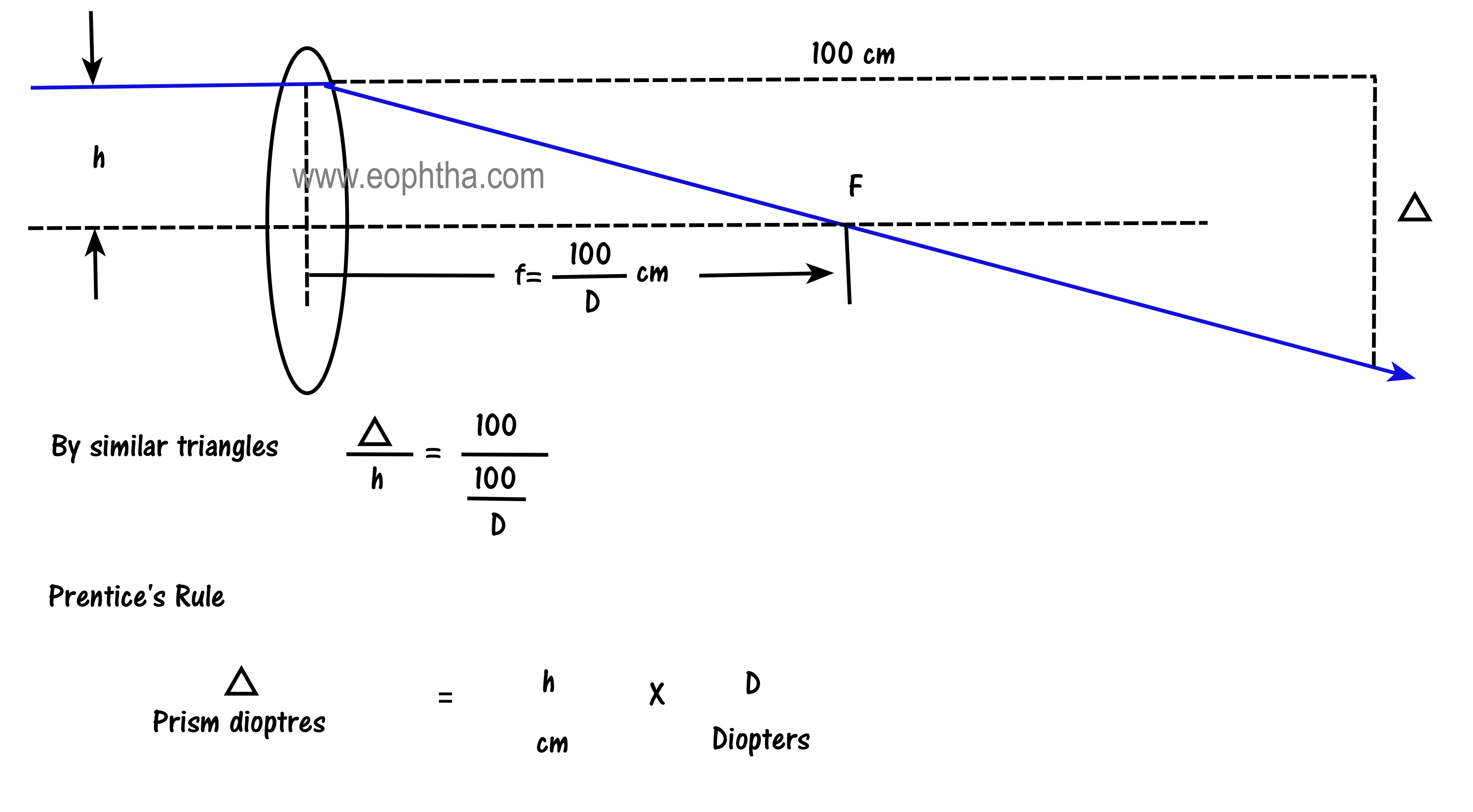
Prismatic Effect of Lenses (Prentice’s rule)
A lens has no prismatic power at its optical center. A ray passing through the optical center of a lens passes through undeviated. The prismatic power of a lens at any point on the lens is equal to the distance of that point from the optical axis in centimeters multiplied by the power of the lens in diopters. This is called as the Prentice’s rule. The decentration or the distance in cm away from the optical center of the lens is routinely made use of while making glasses in the optical dispensary.
Prismatic Effect of Glasses on Strabismic Deviations:
- Plus lenses decrease the measured deviation, whether esotropia, exotropia or hypertropia.
- Minus lenses increase the measured deviation, whether esotropia, exotropia or hypertropia.
The true deviation is changed by approximately: (2.5) (D) %
Where D= the bilateral spectacle lens power
For example, an exotrope of 40 PD wearing -10.00 DS glasses will measure
(2.5) (10) = 25 % more exotropia, for a total of 50 PD of exotropia.
Remember 3M mnemonic: Minus Measures More
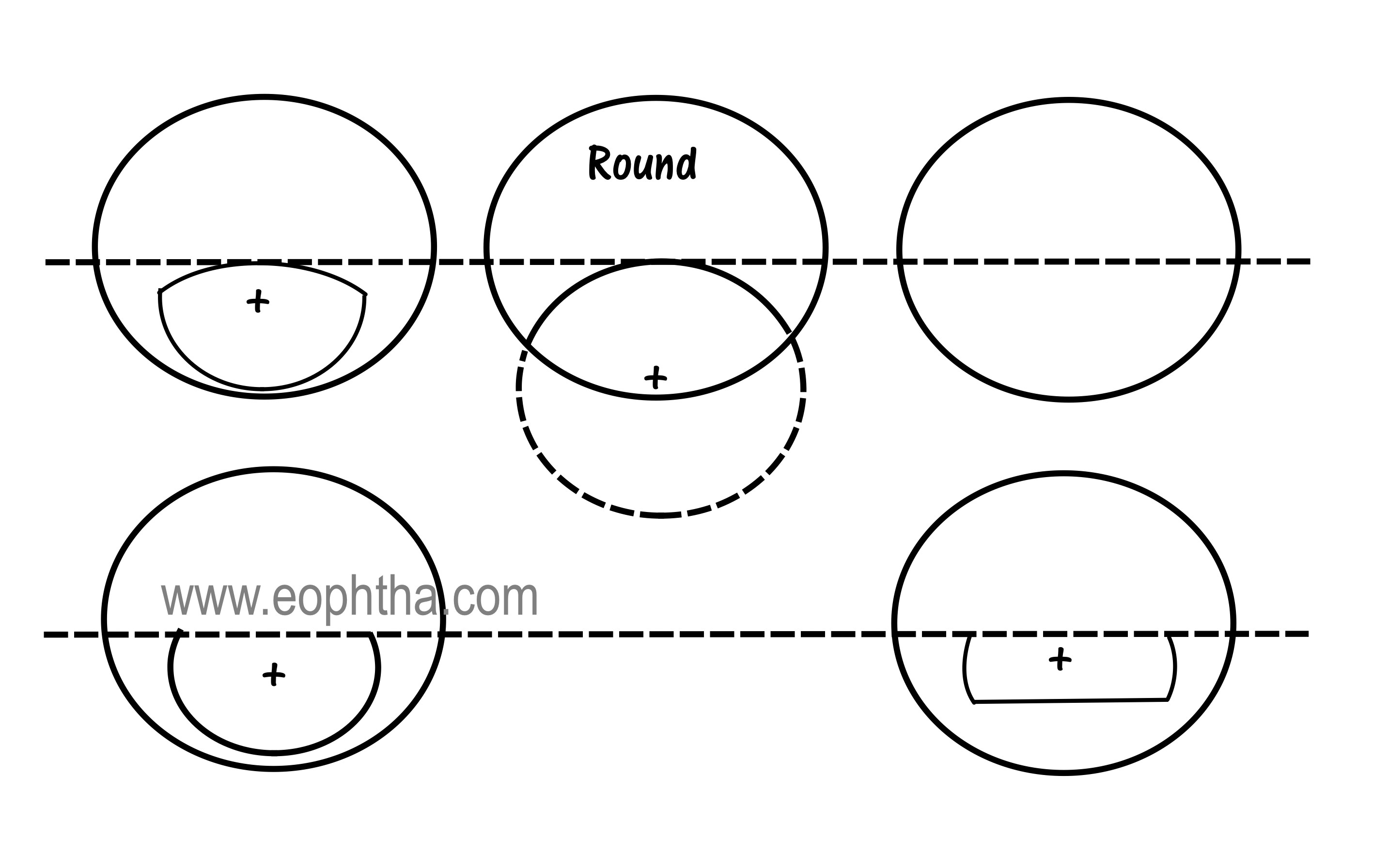
Bifocal Segments – Prismatic Effects
The optical centers of the bifocal segments are denoted by the cross symbol. If the optical center of the segment is at the top of the segment, there is no or minimal image jump. The Round-top segment have maximum image jump as the optical center is at the bottom of the segment and Franklin (Executive) segment has no image jump as the optical center is at the top of the segment.
What is IMAGE JUMP?
It is produced by the sudden introduction of prismatic power at the top of the bifocal segment. The object that the eye perceives in the inferior field when looking straight ahead suddenly jumps upward when the eye turns down to look at it.
Fresnel Prisms:
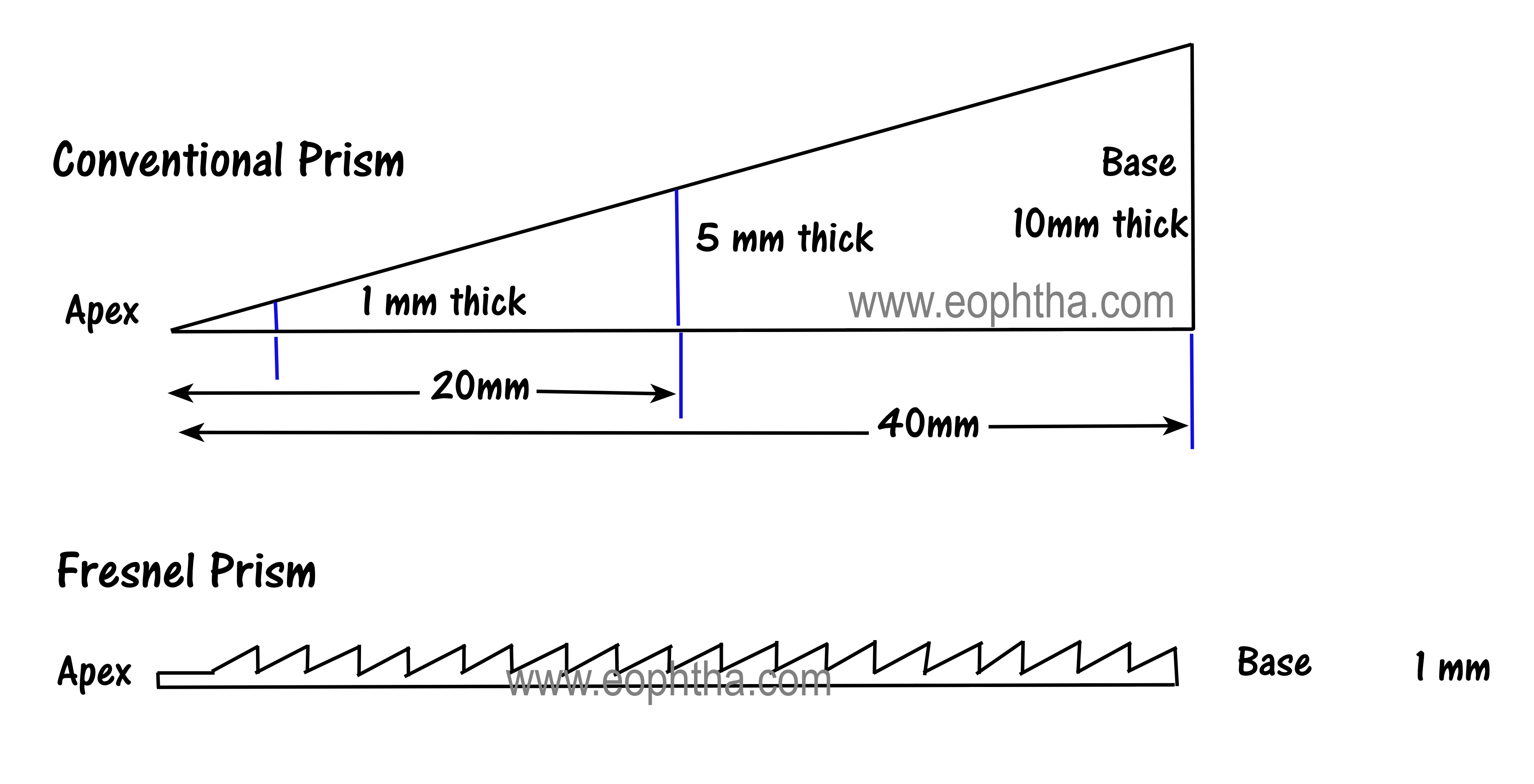
Fresnel prisms are side-by-side stacked up linear strips of long, narrow, thin transparent prisms. Plastic Fresnel prisms are available as press-onTM prisms from 0.5 to 40 PD for application to the rear surface of spectacle lenses. They are convenient and lightweight but are difficult to clean, requiring periodic replacement. When prisms of larger strengths (more than 6 PD) need to be prescribed, Fresnel prisms are used.
Oblique Prisms:
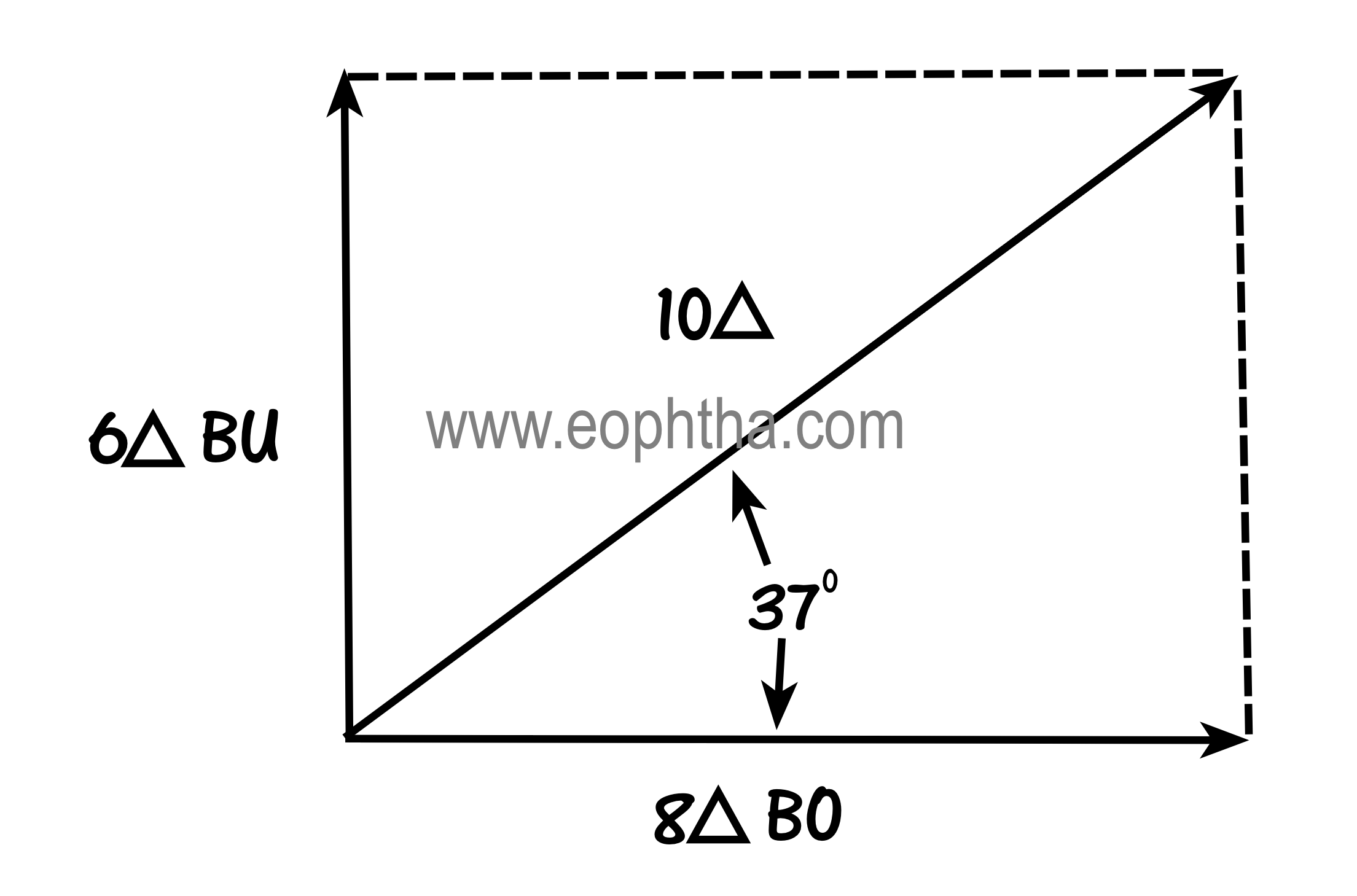
Horizontal and vertical prisms may be combined into an oblique prism by ordinary vector addition. Prescribing oblique prism saves weight, thickness, and cost in spectacles. In this case, for the left eye, an oblique Fresnel prism of 10 PD base up and out in the 37-degree meridian can be given instead of two prisms 6 PD base-up and 8 PD base-out.
Prisms and Chromatic Effects: Prisms split white light into its component colors because the refractive index of transparent materials is slightly different for a different wavelength of light.
Applications of Prisms in Ophthalmology
- PRISM ADAPTATION TEST: In patients with partially accommodative esotropia, press-on base out prisms are prescribed over full hyperopic correction. The patient is reviewed in approximately 2 weeks. If esotropia has increased, then the prisms are increased. This continues at 2 weeks interval until the angle is stabilized. The surgeon operates on the full prism adapted angle to reduce the under-correction rate.
- VERTICAL PRISM TEST: It is used to assess fixation preference in children with straight eyes. The test is performed by placing 10 – 15 PD prism base -up or base-down in front of one eye, thereby producing vertical strabismus. A 15 PD base-down prism placed over the fixating eye causes both eyes to elevate. There will be no movement of either eye when placed in front of the amblyopic eye.
- PRISM ALTERNATE COVER TEST: The prism alternate cover test determines the amount of prism necessary to neutralize the full deviation including any latent phoria. The test is performed by first using the alternate cover test to estimate the size of the deviation. A prism is then placed over one eye oriented appropriately in an attempt to neutralize the deviation. Alternate cover testing is then performed with the prism in place until there is no refixation.
- SIMULTANEOUS PRISM COVER TEST: The simultaneous prism cover test is used to measure the tropia component of the monofixation syndrome without dissociating the phoria and therefore used in small-angle strabismus. The first step is to estimate the size of tropia by the Hirschberg test. A prism as determined by estimating the size of tropia is then presented in front of the non-fixing eye to neutralize the tropia, as the fixing eye is simultaneously covered by an occluder.
- MEASURING VERGENCE AMPLITUDES: Fusional convergence and divergence amplitudes are measured using the prism bar. The patient is made to fix at a target at distance or near depending on the distance at which the amplitude is being measured. Base –out prism bar is placed in front of one eye in increasing steps until the patient reports diplopia or inability to fuse. Base-out determines convergence and base-in determines divergence amplitudes.
- TO DETECT ANOMALOUS RETINAL CORRESPONDENCE(ARC): A thin red strip of glass on top of a prism is used to detect ARC. A patient with ARC will complain of paradoxical diplopia on the red glass test after prism neutralization. An esotropic patient will complain of crossed diplopia and an exotropia will complain of uncrossed diplopia with prism neutralization with red glass test if there is ARC.
- PRISMS FOR DIPLOPIA: To relieve diplopia and increase the field of binocular single vision in incomitant strabismus. Prisms are prescribed to neutralize deviations and thereby relieve diplopia in primary position if there is paralytic or restrictive strabismus.
- PRISMS FOR AHP IN NYSTAGMUS: In nystagmus, anomalous head posture is often adopted to place eyes in the null position. Prisms place eyes in this position, abolishing the need for anomalous head posture. This can be used as a trial before Kestenbaum surgery for nystagmus.
- PRISMS FOR FIELD DEFECTS: In patients with tubular vision or homonymous hemianopia, prisms are used to reorient the field of vision.
- PRISMS FOR EXERCISING: In convergence insufficiency (CI), prisms are used for improving convergence. Base out prisms exercises the eyes with CI.
Ophthalmic Instruments that use Prism:
- Slit-lamp
- Koeppe's Gonio lens
- Haidinger brushes
- Applanation tonometer
- Keratometer
- Exophthalmometer
- Indirect ophthalmoscope
- Phoropter
- Synaptophore
- Pupillometer
- Operating microscope
Puzzle
Since the basic lesson on prisms is over let us solve a prism puzzle now.A 10 PD prism is placed BASE IN before the left eye of a patient with perfectly straight eyes (orthotropia) at a distance and near.
A. Which way will a distant object appear to move, to the patient's left eye, when the prism is introduced?
B. Which way will the patient's left eye appear to be displaced to an examiner sitting facing the patient?
C. If the prism is held 2 cm from thepatient's eye, how far does the patient's eye appearto be displaced to the examiner?
D. Will the patient have to converge or diverge to compensate for the prism?
E. What type of deviation will be apparent to the examiner by the cover - uncover testing, with the prism in situ?

Answers:
A. The image will move to the left towards the apex of the prism. The image seen by the patient is a virtual image and virtual images are displaced towards theapexof the prism. Note that the retinal image is a real image and that is displacednasallytowards thebaseof the prism.
B. The left eye would appear to be displacedTEMPORALLY, again towards the apex of the prism. The examiner's view of the patient's eye is also a virtual image, again displaced towards the apex of the prism.
C. 2mm.This is because a 10 Prism of deviation displaces light rays 10 cm at 100 cm from the prism. Therefore, the displacement at 2cm is
(2/100) x10cm =0.2 cm=2mm
D. Diverge because the line of sight has been directed inward by the prism.
E. The patient will have esophoria on the cover- uncover testing, for the fusion- free position measured anterior to the prism is an esodeviation
Prisms are an integral part of ophthalmology. Concepts need to be well understood which makes prescription of prisms an easy game for anyone and it will definitely be a game-changer for your tricky troublesome patients!