
Blepharoptosis refers to the inferodisplacement or drooping of the upper eyelids.The condition can be congenital associated with the presence of a dystrophic levator muscle or acquired due to a myogenic, neurogenic, mechanical, aponeurotic or traumatic cause. We aim to provide certain general guidelines to the management of a patient with ptosis. In assessment of long case of ptosis the clinical examination should start with History as with any other case.
History:
Obtain a thorough medical and ophthalmic history.
- The onset of ptosis,
- Alleviating or aggravating factors,
- Family history of ptosis
- Whether increasing, decreasing, or constant since the time of manifestation
- Association with
- Jaw movements
- Abnormal ocular movements
- Abnormal head posture
- History of
-
- Trauma or previous surgery
- Poisoning
- Use of steroid drops
- Any reaction with anesthesia
- Bleeding tendency
-
- Previous photographs may prove to be of great help.
Ocular Examination:
- Head Posture:A significant head posture (usually chin elevation as the ptosis is minimum in downgaze in a patient with congenital ptosis) is also one of the indications for surgery especially in the pediatric age group. Abnormal brow position also indicates the functional fall-outs of this condition.
- Ocular Motility:Ocular motility assessment is of utmost importance. It not only is of importance in causes of myogenic ptosis, but the presence of strabismus, especially vertical strabismus entails that it be corrected prior to the correction of the ptosis.
- Visual acuity– Best-corrected visual acuity should be assessed to record any amblyopia if present, especially in cases of congenital ptosis.
- Pupillary Examination:Examination of the pupils is of utmost importance as they are of both diagnostic and therapeutic significance. Diagnosis of conditions like Horner’s syndrome are dependent on the pupillary examination while the presence of pupillary involvement in a case of third nerve palsy can have great prognostic importance for the appropriate management of the case.
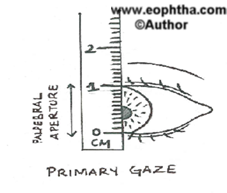
- Thepalpebral fissure- the distance between the upper and lower eyelid in vertical alignment with the center of the pupil.
Normal – 9-10mm in primary gaze
Should be seen in up gaze, downgaze and primary gaze
Amount of ptosis =difference in palpebral apertures in unilateral ptosis or Difference from normal in bilateral ptosis
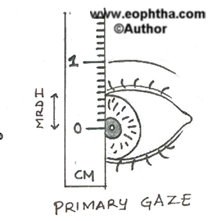
- The marginal reflex distance-1 (MRD-1)- the distance between the center of the pupillary light reflex and the upper eyelid margin with the eye in primary gaze. A measurement of 4 - 5 mm is considered normal. It is important to crosscheck the amount of measured ptosis lest the palpebral aperture may be giving false value due to abnormal positioning of the lower lid.
Amount of ptosis
The difference in MRD 1 of the two sides in unilateral cases or the difference from normal in bilateral cases gives the amount of ptosis.
Hold the light source directly in front of the patient looking straight ahead. The distance between the center of the lid margin of the upper lid and the light reflex on the cornea would give the MRD 1. If the margin is above the light reflex the M RD 1 is a +ve value. If the lid margin is below the corneal reflex in cases of very severe ptosis the MRD 1 would be a –ve value. The latter would be calculated by keeping the scale at the middle of upper lid margin and elevating the lid till the corneal light reflex is visible. The distance between the reflex and the marked original upper lid margin in –ve sign would be the MRD 1.

Grading of the severity of ptosis
= 3 mm : moderate ptosis
=or > 4 mm : severe ptosis
It must be remembered that ptotic lid in unilateral ptosis is usually higher in down gaze due to failure of levator to relax.
The ptotic lid in acquired ptosis is invariably lower than normal lid in down gaze.
- The marginal reflex distance-2 (MRD-2)- the distance between the center of the pupillary light reflex and the lower eyelid margin with the eye in primary gaze. A measurement greater than 5 mm is considered normal.
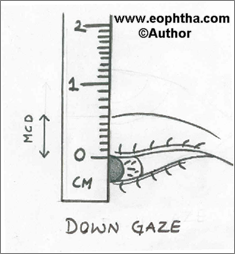
- The margin crease distance (MCD)is the distance from the upper eyelid margin to the lid crease measured in down gaze. In women, a central measurement of 8 - 10 mm is considered normal, and in men, 5 - 7 mm is considered normal.
It helps in planning the surgical incision. In some cases where more than one lid creases are present, the most prominent one should be considered. (Fig. 3)
- Levator functionis the distance the eyelid travel from downgaze to upgaze while the frontalis muscle is held inactive at the brow.
Berke’s Method (lid excursion):
Lid excursion is a measure of the levator function. The frontalis action is blocked by keeping the thumb tightly over the upper brow and asking the patient to look up from down gaze and measuring the amount of upper lid excursion at the center of the lid. (Fig. 4a,b)

Grading of levator action
< 4mm – poor levator function
5-7 mm – fair levator function
8-12 mm – good levtor function
The normal levator function is between 13-17mm
Putterman’s method
This is carried out by the measurement of distance between the middle of upper lid margin to the 6’o clock limbus in extreme up gaze. This is also known as the Margin limbal distance (MLD).
Normal is about 9.0 mm
The difference in MLD of two sides in unilateral cases or the difference with normal in bilateral cases multiplied by three would give the amount of levetor resection required.
Assessment in Children
Measurement of levator function in small children is a difficult task, as the child allows no formal evaluation. The presence of lid fold and increase or decrease on its size on the movement of the eyelid gives us a clue to the levator action. The presence of anomalous head posture like the child throwing his head back suggests a poor levator action.
Iliff Test
This is another indicator of levator action. It is applicable in the first year of life. The upper eyelid of the child is everted as the child looks down. If the levator action is good lid reverts on its own.
10. Themargin fold distanceis the distance from the upper eyelid margin to the fold of the skin. This is also referred to asshow. It forms an important landmark during ptosis repair.
11.Bell’s responseshould be assessed and lower eyelid laxity or scleral show should be appreciated which may alter the amount of ptosis repair. Confirmation of the presence of Bell’s phenomenon is important before undertaking any surgical procedure to avoid the risk of postoperative exposure keratopathy. It is the upward rotation of eyeball on the closure of the eye. This is referred to as Bell’s positive.

Fig 5: Assessing Bell’s phenomena.
12. The presence or absence of corneal sensations should be noted using a cotton wisp (Fig 6)
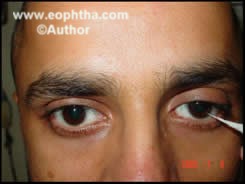
Fig 6: Assessing the corneal sensation.
13. Eyelid retraction may warrant thyroid function studies and the consideration of dysthyroid orbitopathy.
14. Parinaud syndrome should be considered if convergence-retraction nystagmus and pupillary light-near disassociation is found in conjunction with eyelid retraction; neuroimaging should be obtained.
15. The presence of proptosis in other eyes may give the appearance of pseudoptosis. Pseudoptosis can also result from microphthalmos, enophthalmos or anophthalmos, acquired hypotropia after a blowout fracture (orbital floor fracture), superior sulcus deformity, or contralateral vertical lid retraction.
Important points which would help you in Differentiating between a case of congenital and acquired ptosis
The history of the patient is usually definitive which is helpful in establishing the diagnosis.
Important points in favor of congenital simple ptosis is that the ptosis classically decreases in downgaze as the dystrophic levator muscle is neither able to contract nor to relax. Hence the measurements of the palpebral aperture in downgaze in the ptotic eye may at times be more than that in the contralateral normal eye in cases of unilateral ptosis.
The upper eyelid crease is weak or absent in a case of moderate to severe congenital ptosis while in cases of acquired ptosis of a similar degree, the crease is higher than usual.
Associated synkinesis is usually present with congenital ptosis. However, at times cases like congenital third nerve palsy with aberrant regeneration of the nerve may pose to be an important diagnostic dilemma.
Variability and intermittency of symptoms usually indicates myasthenia. This history should be evaluated in every case of ptosis.
Similarly, history of diplopia and the presence of ophthalmoplegia on examination indicate conditions like chronic progressive external ophthalmoplegias and warrant investigations for the same.
Laboratory Studies:
If myasthenia gravis is suspected following may be needed:
- Serum assay for acetylcholine receptor antibodies
- Edrophonium chloride (Tensilon) test
- Single-fiber electromyography
- Repeated nerve stimulation test
In patients with chronic progressive external ophthalmoplegia following should be considered:
- Electrocardiogram
- Electroretinogram
- Electromyography
- Mitochondrial assay
Patients with suspected thyroid abnormalities should undergo tests for thyroid function including
- triiodothyronine (T3),
- thyroxine (T4),
- thyroid-stimulating hormone (TSH), and
- Imaging Studies
Other Tests
Tensilon Test
This test is done in doubtful cases where acquired ptosis due to Myasthenia Gravis is suspected. In adults, 1 mg of neostigmine is injected I/M. The ptosis improves in 5 to 15 minutes if Myasthenia gravis is the cause. Alternately 10 mg of edrophonium may be injected I/V. It is loaded in a tuberculin syringe and 2mg injected slowly in 15-30 seconds. The needle is left in situ and rest injected slowly if no untoward incident is observed. The effect occurs in 1 to 5 minutes if myasthenia is the cause. If cholinergic reaction occurs 0.5mg of atropine is given I/V.
Phenylephrine test
Sympathomimetic agents can be used to stimulate the Mueller muscle, as follows:
2.5% phenylephrine
10% phenylephrine: Be aware of cardiac complications.
0.5% apraclonidine: an alpha-adrenergic agonist.
1.0% apraclonidine: an alpha-adrenergic agonist.
Instill 2 drops on the eye under the eyelid (have the patient look down), wait 5 minutes, and assess any change in the palpebral fissure and the marginal reflex distance.
If no response is observed or if elevation is not adequate, external levator resection or advancement may be needed to correct the blepharoptosis.
If a good response is observed, the ptosis can be repaired by Mueller muscle–conjunctival resection.
Phenylephrine 10 % drops are used to assess mild cases of ptosis. The positive phenylephrine test suggests that the patient would respond well to Muller’s muscle resection.
Jaw movements
The presence of jaw winking is assessed by moving the jaw from side to side (chewing movements), opening and closing the mouth.
Traction test
The lashes are held between the thumb and forefinger and traction applied. We look for the downward movement of the eyeball to rule out surgical or traumatic adhesion of upper lid with the globe. If the lid and the eye move independently no adhesion exists.
After all the history and examination you may classify ptosis as:
A. Congenital Ptosis
- Congenital simple ptosis
- With oculomotor abnormalities (Superior Rectus muscle underaction; Double elevator palsy).
- Ptosis associated with the Blepharophimosis syndrome
- Synkinetic ptosis (associated with abnormal neural connections)
- Marcus Gunn Jaw Winking
- Misdirected third nerve ptosis
B. Acquired Ptosis
- Myogenic (Myasthenia gravis; CPEO)
- Neurogenic (Third Nerve palsy; Ophthalmoplegic migraine)
- Mechanical (Lid tumors)
- Aponeurotic
- Traumatic
C. Pseudoptosis
- Decreased intraorbital volume as may be associated with microphthalmia, anophthalmia, phthisis bulbi etc.
- Superior sulcus abnormality secondary to trauma or other causes.
- Ipsilateral hypotropia with the contralateral fixating eye.
- Contralateral lid retraction.
- Ipsilateral dermatochalasis or blepharochalasis
Before we take up the surgical issues in management of ptosis, it is important to know the anatomy of the upper eyelid and brow.
Surgical Anatomy of the upper eyelid and eyebrow
A thorough understanding of the surgical anatomy of the eyelid is necessary to give good functional and cosmetic results. The layer of upper eyelid from anterior to posterior are skin, subcutaneous tissue, orbicularis muscle, submuscular tissue, orbital septum and preaponeurotic pad of fat, levator aponeurosis, muller muscle, tarsal plate and conjunctiva (Fig 7).Skin of the upper lid is thinnest in the body. The skin is attached loosely over the eyelid, but firmly over the brow, lid margins and canthi.Orbicularis muscle is responsible for blinking and lid closure. It originates from medial palpebral ligament and the fibres spread in elliptical fashion. It is divided in to orbital and palpebral portion. The palpebral portion runs from medial canthal ligament to lateral palpebral raphe. Submuscular layer is corrected with the submuscular layer of the brow and thus the infection can spread through this plane. Most of the blood vessels and nerve lie in this area. Orbital septum and tarsal plate form a continuous layer of fibrous tissues and is mainly responsible for the stability of the eyelid. Levator muscle is the main retractor of the upper eyelid. It originates above the optic foramina under the lesser wing of sphenoid. It moves forward under the orbital roof and above the superior rectus muscle. Near the equator of the globe it is transformed in to fibrous aponeurosis, which travels forwards and inferiorly and gets inserted into the upper 2/3rd of the anterior tarsus. The other attachments of the levator aponeuresis are to skin of the upper lid after penetrating the orbicularis muscle forming the lid crease. Its medial and lateral extensions are known as ‘horns’. The lateral horn attaches to the orbital tubercle. by the canthal ligament. It is important to remember that the lateral horn separate the lacrimal gland into palpebral and orbital part. The medial horn forms the medial canthal ligament.

Fig. 7: Showing surgical anatomy of the eyelid.
Muller muscle is a thin sheet of non-striated muscle which arises near the junction of the levator and its aponeurosis from its under surface and attaches to the superior forward border of tarsus. The superior transverse ligament (whitnall’s ligament) arises from the under surface of the levator. It assists in suspension of the levator muscle. Conjunctiva is inner most layer of the lid. The palpebral conjunctiva is transparent, highly vascular and is strongly attached to tarsus of upper lid. It is continuous with the bulbar conjunctiva via superior fornix. Frontalis muscle originates from epicranial aponeurosis anterior to the coronal suture and inserts into skin and subcutaneous tissue of the eyebrow. It helps in elevation of upper lid by drawing the scalp, raises the eyebrow and forms the crease on forehead.
Timing of Surgery
If possible it is advisable to wait till 3-4 years of age in cases of congenital ptosis. The following advantages are obtained:
- Better assessment is possible
- Tissues are better developed to withstand surgical trauma
- Better post-operative care is possible due to better co-operation
There should be no delay in surgical management in cases of severe ptosis where pupil is obstructed (8a,b). The latter may cause amblyopia. Delay should also be avoided in cases of bilateral ptosis where child is likely to develop bad postural habits like head tilt, brow wrinkling, eyebrow arching or odd facial grimaces which are difficult to eradicate later. In these cases a temporary procedure may be opted early on followed by definitive surgery later.
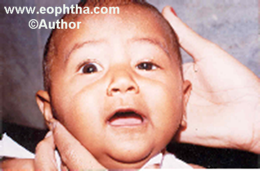
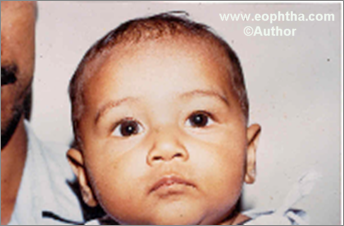
Figure 8: Use of temporary sling in severe ptosis.Pre-operative ptosis left eye. Following a temporary sling procedure.
Choice of Surgical Procedure
The choice is determined by:
- Whether the ptosis is unilateral or bilateral
- Severity of Ptosis
- Levator action
Simple ptosis or associated anomalies
COMMONLY PERFORMED SURGERIES
Fasanella Servat Operation
Levator resection
Brow suspension ptosis repair
Indications for The Choice of Different Surgical Procedures
|
Ptosis |
Levator action |
Surgery |
|
Mild |
> 10 mm |
Fasanella Servat or small levator resection |
|
< 10 mm |
Levator resection |
|
|
Moderate |
Good |
Levator resection |
|
Fair |
Levator resection |
|
|
Poor (rare) |
Whitnall’s sling or Brow suspension |
|
|
Severe |
Fair |
Levator resection or Brow suspension ptosis repair |
|
Poor |
Brow suspension ptosis repair |
SURGICAL TECHNIQUES
Modified Fasanella Servat surgery
It is the excision of tarsoconjunctiva, mullers and levator. One of its modifications that we use the procedure is as follows.
Xylocaine with adrenaline is used for local anesthesia. The lid is everted and tarsal plate exposed. Three sutures are passed close to the folded superior lid margin at the junction of middle, lateral and medial one-third of the lid. Three corresponding sutures are placed close to the everted lid margin. The proposed incision is marked on the tarsal plate such that a uniform piece of tarsus not exceeding 3 mm is excised. A groove is made on the marked line of incision and the incision is completed with the scissors (Fig. 9). The first set of sutures help in lifting the tarsal plate for excision. The second set aids suturing by lifting and supporting conjunctival and tarsal edges during suturing.
5-0 plain catgut is used for continuous suturing and the knot buried under the wound. Antibiotics are instilled and pad and bandage done. Post-op patients are kept on antibiotics and anti-inflammatory agents and cornea observed for any sign of abrasion and treated accordingly if needed.

Fig. 9
Levator resection
This is the most commonly practiced surgery for ptosis correction. It may be performed by skin or conjunctival route but the former is preferred by most surgeons because it is universally applicable and allows a good titration/assessment on the table. (Fig 10)

The proposed lid crease is marked. Xylocaine with adrenaline is locally infiltrated. The injection is also used in cases being operated in general anesthesia to help in hemostasis.
Three sutures are passed near the lid margin to provide traction. A lid spatula placed under the lid and incision through the skin and orbicularis made along the crease marking. The inferior skin and orbicularis are dissected away from the tarsal plate. The upper edge is separated from the orbital septum. The orbital septum is cut completely exposing the preaponeurotic fat. Fat is retracted exposing the whole tendinous aponeurosis. Three partial-thickness traction suture are passed through the distal end of the aponeurosis. The fibres of the aponeurosis are cut from their insertion. The levator is freed from the adjoining structures. The lateral or the medial horn may be cut where necessary making sure not to damage the lacrimal gland or the pulley of superior oblique muscle respectively. Care should be taken that Whitnalls ligament is not damaged. Three double-armed vicryl 5 – 0 sutures are passed through the tarsus about 2 mm from the upper border in the center and at the junction of central third with the medial and lateral thirds. These sutures are then placed in the levator and intraoperative assessment made. The lid level and contours are evaluated. The eyelid is left at the position determined preoperatively based on the levator action
Levator actionRecommended lid placement
2-4mm 1mm above the limbus
5-7 mm 1 mm below the limbus
8 mm or more 2 mm below the limbus
The sutures are then finally secured. The excess levator is excised. If required a strip of skin is removed from above the lid crease. A piece of orbicularis may be excised inferior to the lid crease to debulk the lid. Four to five lid forming sutures are placed. The sutures pass through skin edges taking a bite through the cut edge of levator.
An inverse 6-0 suture is passed through the lower lid margin over a bolster. The suture is tucked to the forehead to close the eye after the instillation of antibiotic eye ointment and patch applied. Patients are prescribed oral antibiotics and anti-inflammatory agents. The bandage is opened on the first post-operative day and assessed for any exposure keratopathy. The frost suture is removed on the first or second postoperative day if the closure is adequate. The results of the procedure are fairly gratifying. ( Fig. 11a,b,c,d)
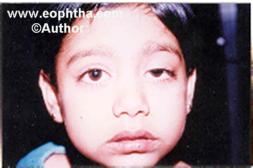



Figure 11 A to D Levator resection procedure pre- and post-surgery photographs
In bilateral cases where the levator surgery is indicated bilateral surgery at the same sitting is advisable to ensure similar surgical intervention in the two eyes. However, in cases where gross asymmetry exists the eye with greater ptosis is operated first followed by the other eye 6-8 weeks later when the final correction of the operated eye can be assessed.
Brow suspension repair
This surgery is the procedure of choice in simple congenital ptosis with a poor levator action. A number of materials like non-absorbable sutures, skin clips, muscle strips, banked or fresh fascia lata strips have been used for suspension. We prefer Poly tetra fluoro ethylene (ePTFE) sutures for temporary thread sling procedure and fresh autogenous fascia lata for permanent brow suspension.
Temporary Sling
Thread sling is carried out in very young children with severe ptosis where the prevention of amblyopia and uncovering the pupil is the main aim. We use CV 0 ePTFE (Goretex) sutures by the modified Crawford technique for brow suspension (Fig. 12). The suture sling procedures have a relatively higher recurrence rate or may show the formation of suture granuloma. Definitive surgery may be performed at a later date when a fascia lata sling is carried out.

Fig. 12 Temporary Sling
Fascia Lata Sling
Fascia lata sling surgery is done in children above four years of age having severe congenital simple ptosis with poor levator action as a procedure of choice.
We prefer fresh autogenous fascia for suspension. Even in cases of unilateral ptosis a bilateral procedure is preferred because a unilateral surgery causes marked asymmetry in down gaze and results of bilateral surgery are more acceptable.
All cases are done under general anaesthesia.. Infiltration with xylocaine and adrenaline is done in the region of the proposed incision in the thigh and the eyelid and the eyebrow region.
Harvesting of fascial lata
A line joining the lateral condyle of femur to the anterior superior iliac spine is marked. An incision is given 2 inches above the lateral condyle on the marked line extending upwards for about one inch. The skin incision is deepened through the fat till the glistening fascia is visible. The fascia is then cleared of the overlying tissue for a length of four inches upwards from the incision. A 12 mm incision is then given at the lower end of the exposed fascia lata. Dissection is then carried out beneath the fascia lata seperating it from the underlying vastus lateralis musclealong the whole length of the previous dissection. Two linear incisions are given 12 mm apart on the fascia along the length of dissection using a long scissors. The superior end of the fascia is made free by making horizontal cut using a long bladed scissors while the assistants retract the skin and the subcutaneous tissue. The subcutaneous tissue is closed using 4 – O chromic catgut and the skin is closed using 4 – O silk sutures. We now have an autologous fascia lata four inches long and 12mm wide. It is kept in a bowl containg Ringer lactate and 1 cc of gentamycin.
The fascia lata strip is kept on a wooden board, stretched and fixed. It is divided into four pieces each of about 3 mm width by a scalpel blade.
Fascia Lata Sling Suspension
Three traction sutures are passed along the lid border. Four incisions are made 3-4mm from the lid border depending on the desired position of the lid fold. The two central incisions are on either side of the center of the lid while the other two are at the junction of middle and lateral thirds and middle and medial thirds of the lid.
The eyebrow incisions are marked next. They are made at a line perpendicular to the intersection of two incisions made laterally and two incisions made medially while the eyelid is placed in the desired normal position. A third incision is made in the middle of the first two but 3-4 mm higher than them.
The eyelid incisions are made down to the tarsus and the brow incisions are made upto the frontalis. Some blunt dissection is carried out to make pockets for the fascial knots. The two ends of a strip are then passed from the outer eyelid incisions to the outer eyebrow incision using a Wright’s fascia lata needle. The needle is passed in the submuscular plain from the lateral brow incision to emerge from the lateral incision in the lid. The fascia is threaded through the eye of the needle and is pulled through. The Wright’s needle is again passed from the lateral incision to the second eyelid incision threaded with fascia and drawn up (Fig 13a). The procedure is repeated on the medial side (Fig. 13b). The fascial strips are pulled up and a single tie is made so as to place the eyelid margins about 2 mm above the desired position as the lids will fall down when the knots are buried (Fig. 13c). After a single tie the position and contour of the eyelid is assessed. Required adjustments are made. Presence of good lid crease is ensured at this stage. The knots are then secured using 5-0 vicryl. A second tie is made and secured.
One end of fascial strip from each brow incision is pulled through the central brow incision. Knots are tied and secured (Fig. 13d). All the knots are buried in the pockets prepared for them. The excess of skin created by shortening of the posterior lamina is judged and excised by removing a spindle of skin from the eyelid crease. Eyelid incisions require no closure. The brow incisions are closed with 4 – o silk and the eyelid crease incision by 6 – O silk.
Patients are prescribed oral antibiotics and antiinflammatory agents. The bandage is removed on the first post-operative day and eye left open. The need for retention of the frost suture is assessed based on the extent of the lagophthalmos and careful monitoring of the cornea for signs of exposure. The thigh sutures are removed after 10 – 14 days.




Fig. 13 A to DFascia Lata Sling Suspension
Management of Complicated Ptosis
Ptosis with oculomotor abnormalities
- In cases with superior rectus involvement (usually associated with severe ptosis) an inferior rectus recession at times combined with superior rectus resection is carried out on the affected side as the first procedure. To correct the ptosis levator resection with bilateral brow suspension is done later.
- Knapps procedure may be done for ptosis associated with double elevator palsy where lateral and medial rectus tendons are transplanted to the area of superior rectus insertion. This does not cause significant limitation of adduction or abduction. Ptosis is corrected 3 months later.
Blepherophimosis syndrome
- Mustarde’s double “Z” plasty with trans nasal wiring is done as a primary procedure.This gives a good surgical result both in terms of correction of telecanthus as well as deep placement of the medial canthus. The results are long lasting.
- Brow suspension is carried out 6 months after the first procedure for correction of ptosis.
Marcus Gunn ptosis
- Mild cases of jaw winking where the jaw winking is minimal can be treated satisfactorily by Fasanella Servat operation while severe cases or cases where jaw winking is prominent, require bilateral resection of levator aponeurosis and terminal levator with fascia lata brow suspension.
Misdirected third nerve ptosis
- In cases of misdirected third nerve ptosis where treatment is imperative levator resection with bilateral fascia lata sling is the procedure of choice.
- Ptosis associated with third nerve palsy is difficult to manage because of poor bell’s phenomenon. A crutch glass may be prescribed or a conservative sling surgery may be performed.
- We hope that you would be able to evaluate, diagnose and properly know how to manage any type of ptosis patient.