
Cataract Surgery is the most common surgery performed all over the world. Proper knowledge of surgical instruments used in cataract surgery is essential. This article gives you an overview and description of instruments commonly used in cataract surgery.
Simcoe's irrigation- aspiration cannula:
Design: Available in two different designs. The original model also called the direct Simcoe where aspiration is through the silicone tube and irrigation through the main hub. The surgeon holds the syringe attached to the silicone tubing which is used to generate suction for aspiration in his/her left hand and the irrigation line is attached to the main central hub. The other model is the Reverse Simcoe where irrigation is through the main hub. The surgeon uses a syringe attached to the main hub to generate suction for aspiration.

Cannulas are available in different sizes: 21,22,23 gauge which has an aspiration port size of 0.5,0.35,0.3 mm respectively. These are 15 mm long in size with an angled front opening.
Some models come with a sandblasted tips for polishing the posterior capsule. The narrow bore ports are useful for the aspiration of fine cortical fibers and get a better hold of tissue, while large bore cannulas are useful for faster aspiration of the bulky cortex.
Advantage: Aspiration of the cortical matter is controlled.
Disadvantage: As the bore is large, it cannot be used in SICS and Phacoemulsification without enlarging the side ports.
Use: Manual aspiration of the lens cortex. It has a dual function of irrigation and aspiration. It can also be used for aspiration of other material from the anterior chamber such as viscoelastic, hyphema, exudates.
Choppers:
Different designs of choppers are available to facilitate cutting and splitting of the lens nucleus which is known as nucleotomy. The choppers facilitate nucleus removal using a two-handed technique holding the chopper in one hand and the phacoemulsification probe in the other. Some choppers have a blunt rounded tip and sharp inner cutting surface for horizontal chopping. Others have a sharp pointed tip for vertical chopping and dividing or splitting the nucleus.
Advantages:
1) More efficient removal of the hard inner nucleus minimizing the phacoemulsification energy as in chopping the critical instrument maneuvers are primarily kinesthetic and are performed with chopper tip( lamellar orientation of the crystalline lens fibers creates natural fracture planes). 2) One does not need the red reflex to visually gauge the depth of the instrument tip. 3) During sculpting, the nucleus is fixated by the capsular bag, in comparison, chopping applies much less force against the zonules because the phaco tip secures the nucleus. 4)Useful in complicated cases like brunescent nuclei, total cataracts, small pupils, weak zonules.
A. Horizontal Chopper:
There are many different horizontal chopper designs, but all feature an elongated tip, which is blunt in order to avoid capsular perforation. A relatively long tip is necessary in order to transect thicker, dense nuclei and the inner cutting surface of the tip may be sharpened for this purpose. Different choppers come with variable angulations of the tip. The classic Nagahara's horizontal chopper comes with a 1.5 mm inner cutting edge and 0.25 mm blunt polished tip. The cutting edge is 90 degrees to the shaft. Angulation of the shaft to handle is 45 degrees. The tip to angle length is 14 mm. The overall length of the instrument is 127mm. It can be used by right or left side port.
Technique: It is called horizontal chop because the instrument tips move towards each other in the horizontal plane during the chop. As the initial step, the central anterior epinucleus should be aspirated with the phaco tip. The chopper tip is entered through the side port made at 1-2 o'clock and it touches the central endonucleus and maintains contact as it is passed peripherally beneath the capsulorhexis edge. This ensures that the tip stays inside the bag as it descends and hooks the endonucleus peripherally. Once it hooked the nuclear equator, the nucleus is deeply impaled with the phaco tip. Then the chopper tip is pulled directly toward the phaco tip, and upon contact, the two tips are moved slightly apart. This separating movement propagates the fracture across the entire nuclear diameter.
The nucleus is rotated and the same maneuver is repeated in order to create a pie-shaped fragment.
Advantage: Better suited for the softer nucleus, highly myopic eyes, vitrectomized eyes.
Disadvantages: Chances of capsular laceration.
B) Vertical Chopper :
Common to all vertical chopper designs, is a short but sharpened tip that is able to penetrate the nucleus. Vertical choppers contain an axe like tip. The axe is 0.75*0.75 mm in dimension. Angulation of the shaft to handle is 45 degrees. Tip to angle length is 10 mm.
Technique: It is called vertical chop because the chopper utilizes a shearing force to split the nucleus vertically into pieces. The initial step is to engage the nucleus with the phaco tip in at least 50% of the nucleus thickness using a high vacuum. Then the axe of the vertical chopper is advanced vertically downwards just in front and adjacent to the phaco tip to create a vertical QUICK CHOP in the nucleus. The phaco tip now moves in upwards and outwards direction to bring the fragment of the nucleus away from the axe , which holds remaining portion of the lens in position converting a cleft into a crack. The final motion is to separate axe and the phaco tip apart to impart a full-thickness crack in the nucleus.
Advantages: Better suited for hard nuclei because it requires the nucleus to be brittle enough to be snapped in half.
Disadvantages: Uses more compressive force so less useful in cases of weak zonules.
DOUBLE ENDED CHOPPER: One end contains horizontal and other end contains a vertical component of the chopper. Many designs available with microfinger pointed vertical or horizontal chopper tip and other end with nucleus rotator. Vertical and horizontal choppers are complementary to each other so double-ended chopper provides both tips on a single instrument.
Keratome (5.1mm)
Design: This is a disposable keratome mounted on plastic handles with angulation of 45 degrees with different designs like straight, bevel up or bevel down. It has a blunt tip. It is 5.1 mm wide with cutting edges on both sides
Instrument:
- Thin triangular blade, bevel up, attached to a polycarbonate handle
- 450 angulation facilitates better visualization
- Width-2.8 – 3.2mm diameter
Uses: To enter the AC after making sclera-corneal tunnel in SICS/PE
- Enter at the centre after depressing the inner lip and seeing the dimple
- Cut with middle 1/3rd of the blade with the blade in a plane parallel to iris plane
- Cut while going IN
For clear corneal incision in PE
4.5 – 5.5mm blunt keratome used to enlarge the tunnel esp while introducing a non-foldable IOL

Use: it is used for extension of a keratome slit for either converting a phacoemulsification case to SICS or for inserting non-foldable IOL.
Disadvantage: It has a blunt tip which can cause Descemet's membrane detachment if not handled carefully.
Shapiro’s Posterior Capsule Polisher
Description: Posterior capsule polisher 23-gauge curved shaft with dual irrigating 0.3 mm tip.
Uses: The posterior capsule may be prepared for lens implantation using this PC polisher after lens cortex aspiration. It can be used to remover fine, sticky cortex adherent to posterior capsule, PC plaque, or small PC cells which can cause obscuration of the visual axis in the post-operative period and early PCO formation.
Forceps in Ophthalmology
Artery forceps/hemostatic forceps ( Not used in cataract surgery, but you must know about this forceps- frequently asked in viva)
Identification
1) Scissor like configuration
2) Blunt tip with multiple straight grooves
3) Stout
4) Locking mechanism at the ring end
.JPG)
Types
1) Large, medium, small (mosquito artery forceps)
2) Straight, curved
Uses
1) To hold bleeding vessels during lid or lacrimal sac surgery
2) To hold skin stay and muscle stay sutures
3) To hold gauze pieces while packing the socket after enucleation or exenteration.
Small artery forceps are commonly used in Ophthalmology
Dastoor’s Superior Rectus Holding Forceps
Identification
1) Toothed
2) S-shaped double curve at the tip (tip is 7.7mm from the fulcrum as the insertion of Superior Rectus is at 7.7mm from limbus)
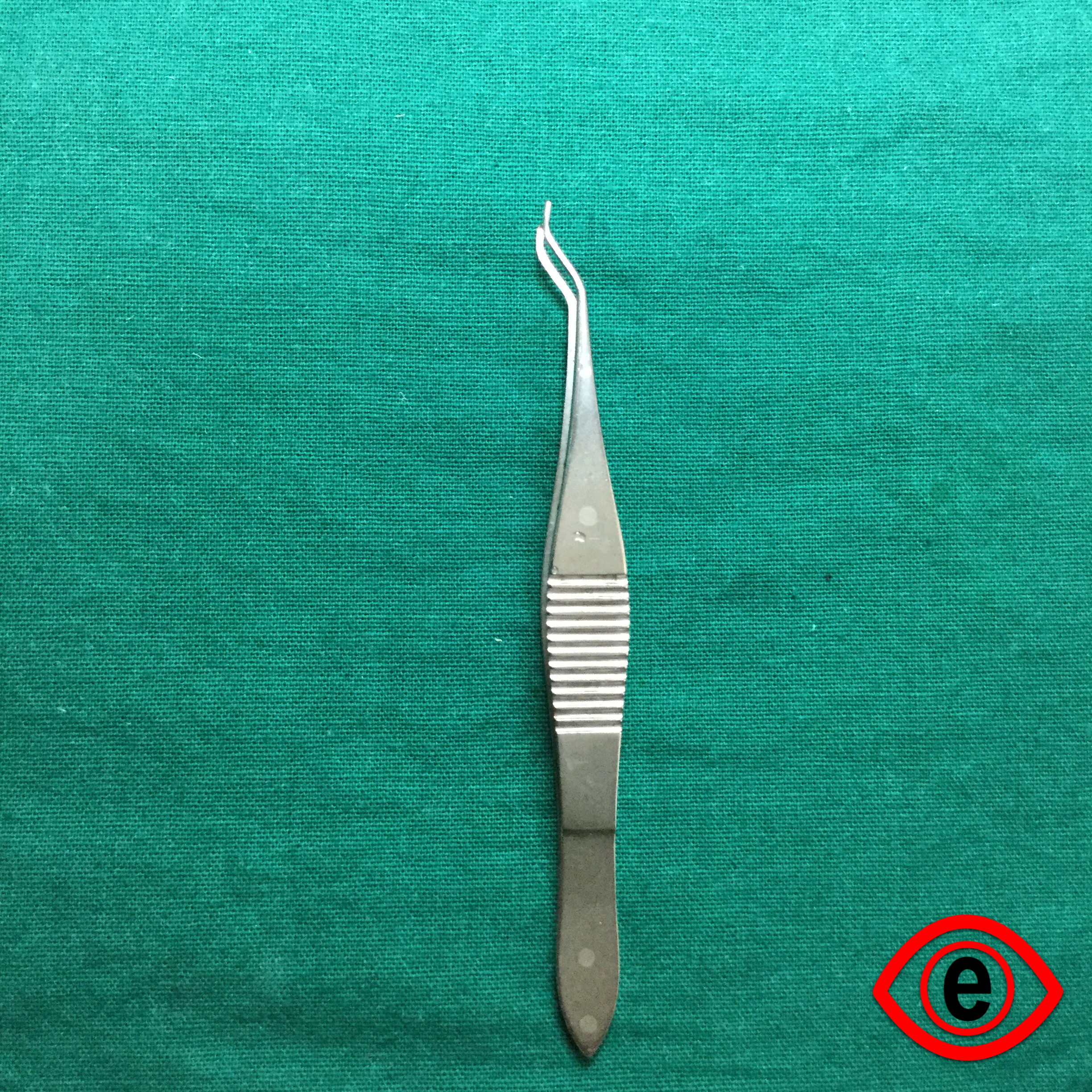
Uses
To hold of MUSCLE BELLIES (mostly superior rectus) of intraocular muscle while passing bridle suture in cataract. Glaucoma and cornea surgeries. Also used commonly in Blumenthal technique of manual SICS to catch the inferior rectus
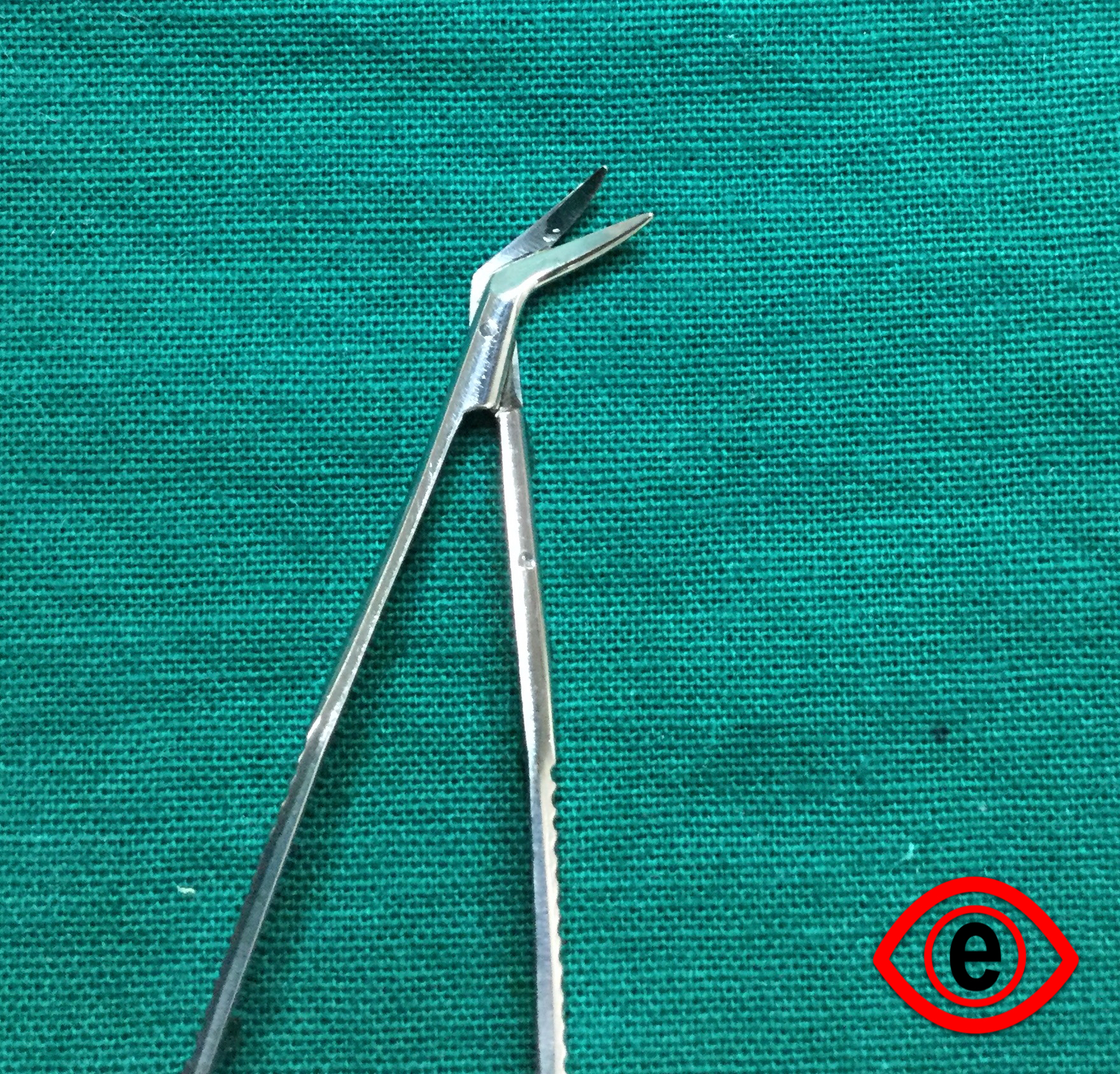
Kelman Mcpherson’s Forceps
Identification
1) Fine
2) Sharp tip
3) Untoothed with angulation
Uses
1) Holding haptic of Intraocular Lens (IOL) during its placement.
2) Used during suturing.
3) For IOL removal.
4) Remove capsular flaps from the anterior chamber.
Lim’s Forceps/Corneoscleral Forceps
Identification
1) Very fine
2) Toothed
Uses: To hold corneal, scleral edges for suturing and for support in various eye surgeries
Pierse Hoskin Forceps
Identification
Tip notched
.JPG)

Uses
To hold delicate tissues
Advantage
Less traumatic
Straight Suture Tying Forceps
Identification
1) Fine limb
2) Untoothed
3) No angulation
Uses
1) To hold fine sutures
2) Used for suture tying, other uses similar to McPhersons
Utrata’s Forceps
Identification
1) Untoothed
2) Sharp tip perpendicular to the body
Uses
1) To tearing capsule / completing capsulorhexis/ removal of capsular tags (USED THROUGH MAIN PORT)
Microcapsulorhexis Forceps
Identification
- Fine
- Sharp tip-act as cystitome
- Forceps like tip
Uses: Capsulorhexis (USED THROUGH SIDE PORT 26G)
Conjunctival forceps
Identification: Fine non-toothed forceps - less traumatic than toothed forceps
Use:
- For grasping conjunctiva
- For stabilizing the muscle prior to weaving the vicryl through the muscle belly in squint surgeries.
Vanna's scissors
Identification - These are very fine, delicate scissors with small cutting blades kept apart by spring action.
Types- 1) Straight 2) Curved
Uses:
- To cut the anterior capsule of lens in ECCE
- To cut the inner scleral flap in trabeculectomy
- To do papillary sphincterotomy
- To perform iridectomy
- To cut pupillary membranes
De Weeker’s scissors
Identification- They are fine scissors with small blades directed at right angles to the arms. The blades are kept apart giving it a v- shape, by its spring action..JPG)
Uses
- To do iridectomy
- To do iridotomy
- To perform manual vitrectomy following a posterior capsular tear.
Corneal scissors ( Castravejo scissors )
Identification -They are fine curved scissors. Their cutting blades are kept apart by spring action. They are available in various shapes and sizes. Blades are angulated to facilitate manipulation and are curved to conform to the curve of limbus.

The blade which is introduced into the anterior chamber is 1mm longer than the outer blade. The longer blade is rounded in the fashion of a spatula to minimize the trauma to corneal endothelium and iris.
The second advantage of longer inner blade is that it does not remove itself from the eye upon each time thereby eliminating the possibility of reintroducing the blade.
Uses
1. To enlarge corneal or corneoscleral incision for cataract and keratoplasty operation
2. To cut the scleral or trabecular tissue in trabeculectomy
Westcott’s scissors
Identification They are stout scissors available with straight or curved blades with sharp or blunt tips.
.JPG)

Blades are kept apart by spring action.
Uses - 1) For cutting and undermining conjunctiva in various ophthalmic surgeries.
2) Can also be used instead of corneal scissors for creating limbal sections.
Stevens tenotomy scissors
Used as an alternative to Westcott scissors
Other Common Instruments
Bard-Parker ® Handle and blade:
Identification:It has a flat handle with a short-grooved neck. Handle no 3 is used in ophthalmic surgeries. No 11-triangular blade and NO 15 – curved elliptical tip blades are fitted with the neck of the handle.
Uses:
To make a groove at the limbus in ECCE
For skin incisions in various lid surgeries, DCR, Chalazion.
For suture removal
Advantage:It forms a guarded section and chance of quick decompression of the globe is reduced.
It can be used for biplanar or triplanar incisions giving rise to secure wounds.
Disadvantages:A conjunctival flap is necessary before creating a section
Iris Repositor:
Identification:It is an elongated S or Z shaped instrument with a stout handle and two long narrow flattened extremities. both the edges and tips are blunt. it’s one end may be curved and other end may be angulated.
Uses:
To reposit the iris in intraocular surgeries
To perform synechiolysis
To fashion the conjunctiva to cover the wound
To check the size and location of anterior chamber entry
To check for vitreous in the anterior chamber
To push the foldable IOL into the bag after delivery from the injector.
Disadvantages:
If repositioning of the iris is not done properly, it can cause
- iris incarceration at the wound
- gaping of the wound
- iris chaffing
- infection
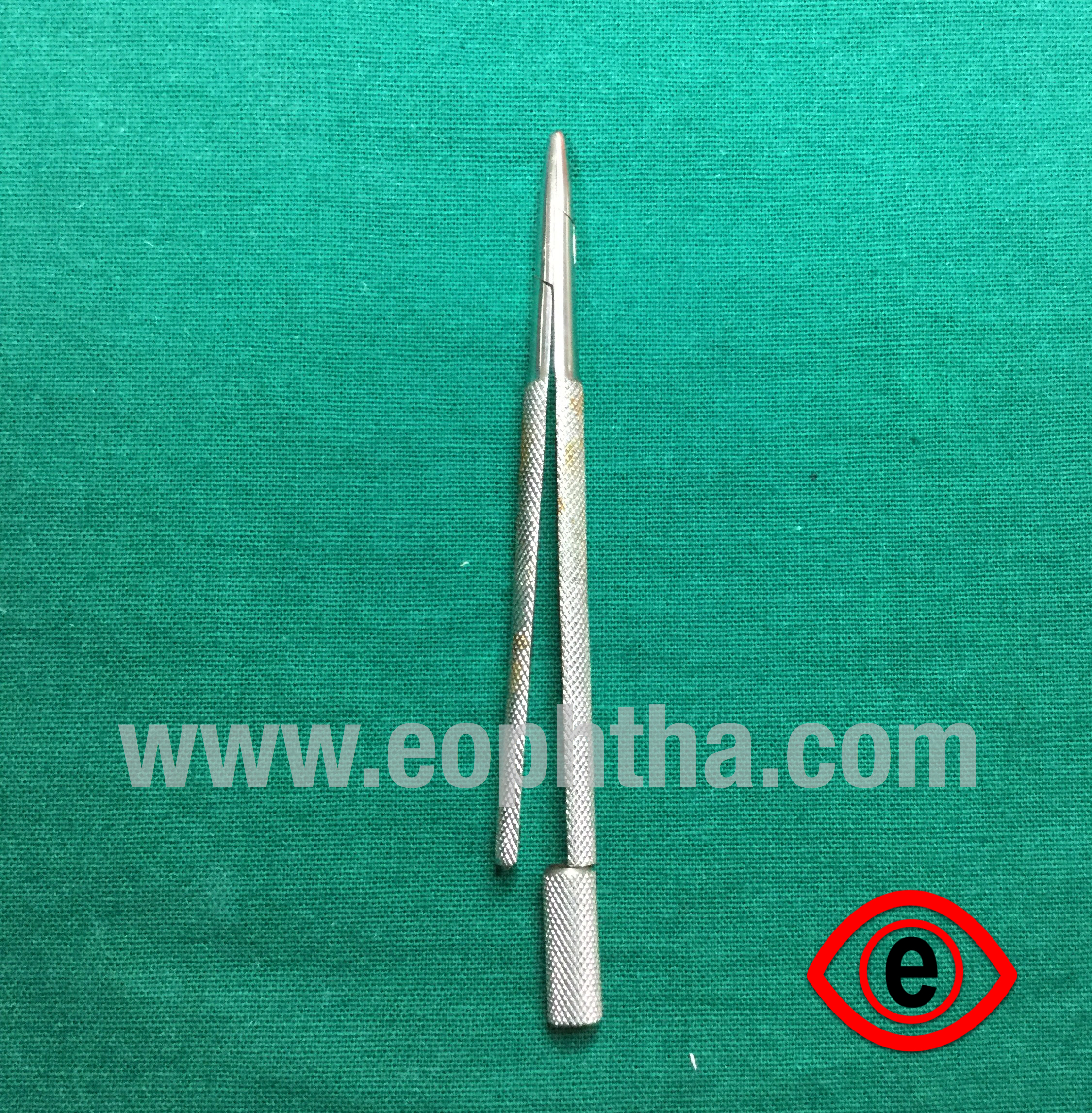
IOL Dialer (Sinsky's hook)
Identification:It is an angular fine hook attached to a long round solid handle. 0.6 mm tip; 10 mm straight shaft; 90-degree hook at tip; manipulating length 120 mm
.JPG)

Use:
To dial IOL for centration in the capsular bag. The hook is positioned in the dialing holes of the optic of IOL or the optic haptic junction and then to rotate in clockwise manner.
It may be used as a left hand/ second instrument during phacoemulsification to rotate, to crack or to chop nucleus.
Disadvantage: It needs careful handling since it can cause PC rent or zonular dialysis if handled roughly.
Eye Speculum
Universal eye speculum
Identification:It has a spring and two limbs with a screw to adjust the limbs. It is called so as it can be used on either eye. When fixed to the eye ball the screw should face outwards.
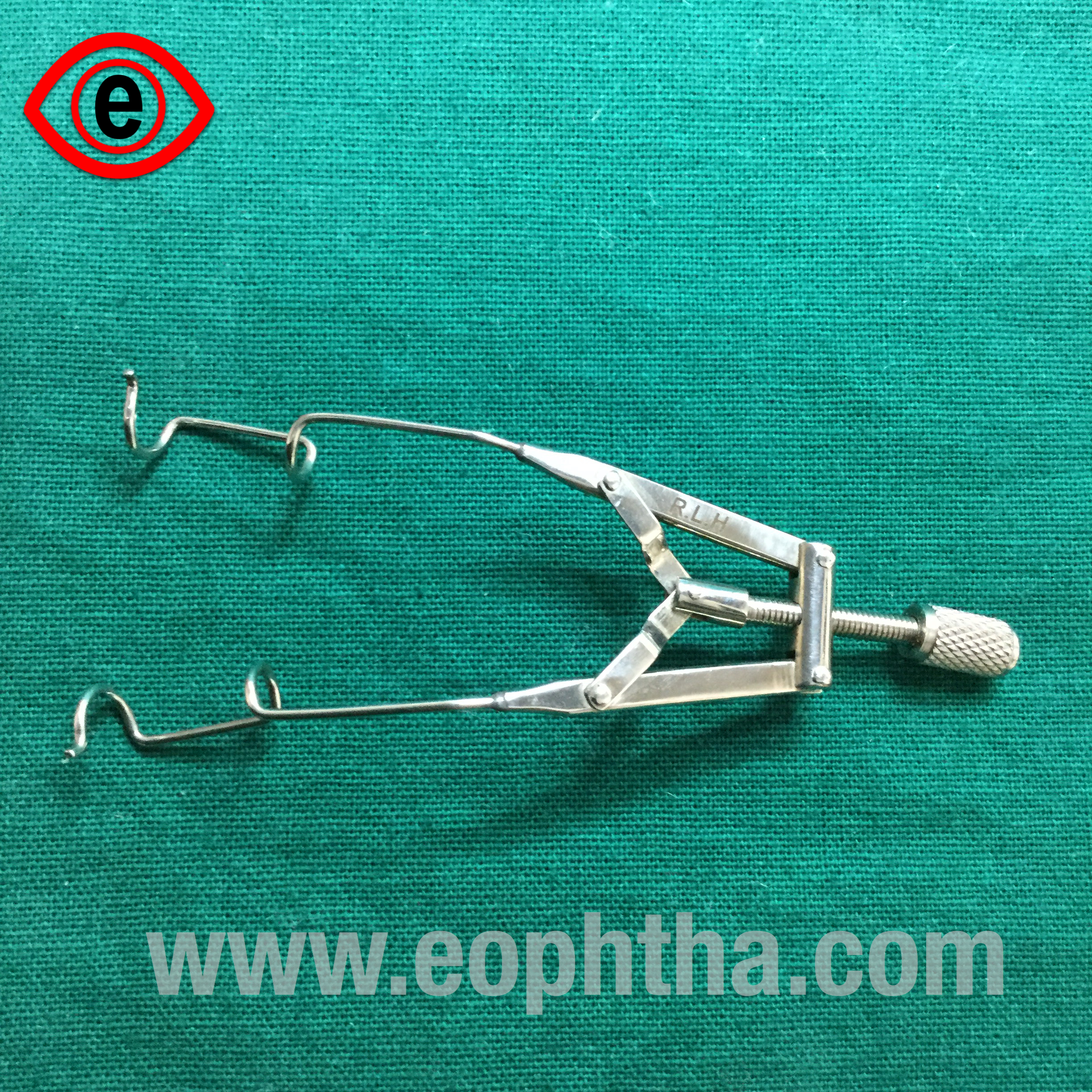
Uses:It is used to separate the lids for good exposure of eyeball mainly during extraocular surgeries. e.g.: pterygium excision, squint surgery, evisceration/enucleation, ocular surface procedures.
Disadvantage:To be used for intraocular surgeries as they tend to increase the intraocular pressure and cause vitreous up thrust and vitreous loss. There is no guard, hence eyelashes can come into the operating field.
BarraquerWire speculum
Identification - It is made up of stainless steel wire with no screw.
.JPG)
Advantage-It is very light so it causes less pressure on the globe so can be used safely during intraocular surgeries.
Bipolar Cautery
Principle:It uses Radiofrequency diathermy technology. The radiofrequency oscillations of the water molecules found within the blood cells generate heat within the vasculature causing coagulation. The current flows along the path of least resistance, between the tips of forceps and the coagulation region, lies between the blade points. A well-defined coagulation patch is achieved by the gentle wiping action of the instrument in a wet field.
Advantage:Limited depth and spread of coagulation.
Coagulation is done with saline which minimizes tissue heating, shrinkage, sticking of coagulum to the electrodes
The ground plate is not required here which is required in monopolar cautery as the current flow is between the bipolar forceps.
Disadvantage:
Sometimes excess power can cause burns, charring, delayed wound healing and more scarring.
Improper earthing can cause shock hazards.
It can cause electromagnetic interference with other operating room devices.
The bipolar cautery is connected to electrically isolated front panel output jacks through a flexible, two conductor, electrical cable.
Kaltz Needle holder
Description:Special pointed ends of Kaltz needle holder help in providing for a better grip of needles with locking handle. The overall length is 140 mm.
Uses:
Used in ophthalmic surgery for holding needles, to suture relatively larger structures like lids and superior rectus.
Also is used to prepare cystitome with 23 gauge needle
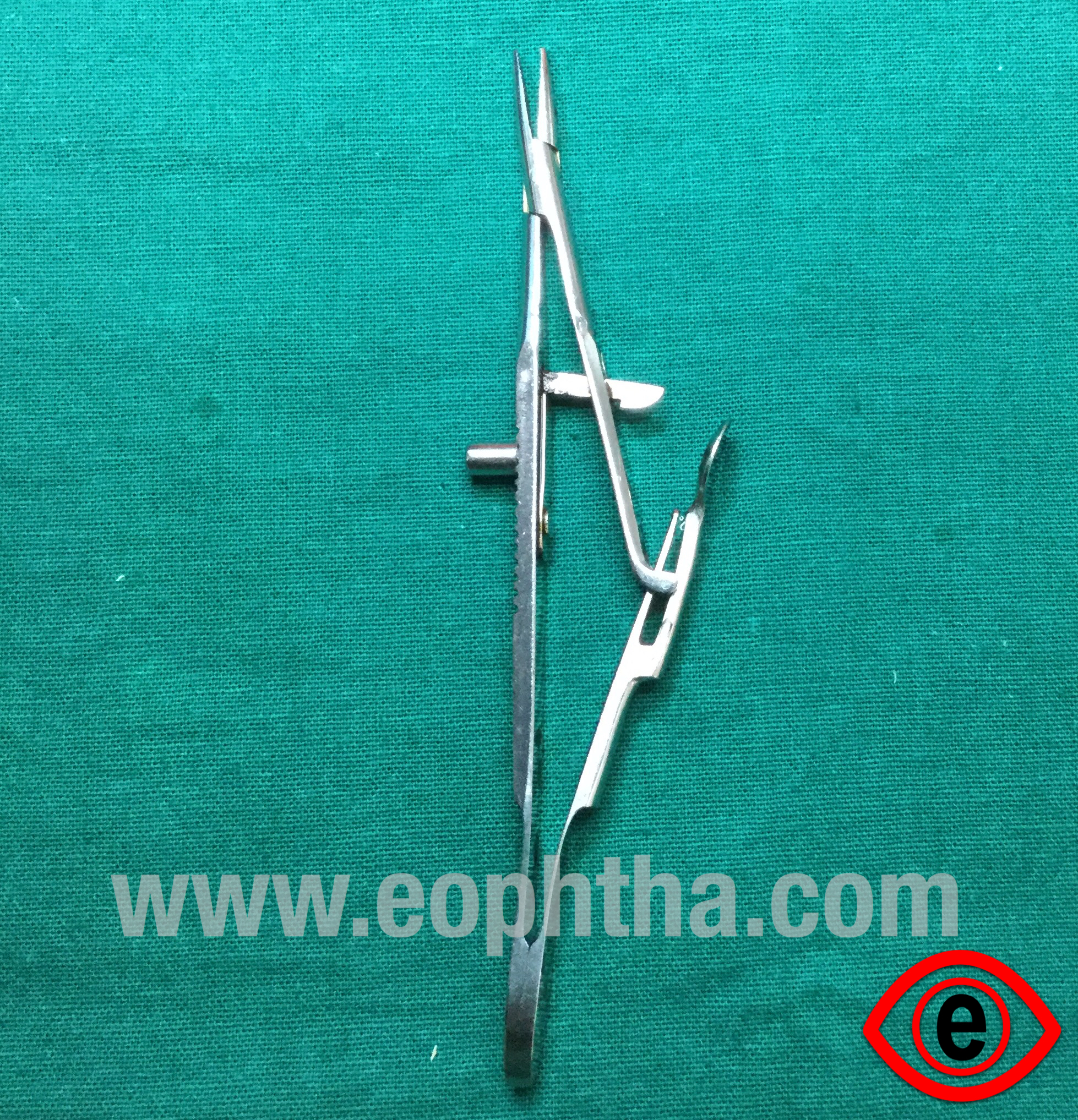
Baraquer's needle holder
Description:It has a smooth jaw which is curved as well as straight. It does not have a locking handle.
.JPG)

Advantage:
Good balance and lightweight.
It offers desired strength and stability.
Uses:
For holding fine needles for 8-0 and 10-0 sutures
May be used for preparing cystitome if Kaltz needle holder is not available
Instruments used in SICS
AC Maintainer:
Instrument specifications:
- Thin hollow metal tube with a beveled end
- Internal diameter: 0.6mm
- External diameter: 1.1mm
- 20G
Uses: To maintain the anterior chamber during various cataract surgeries (esp SICS) usually attached to a bottle of irrigating solution (NS/RL/BSS) and fixed at 6 0’clock.
|
Bottle height (cm) |
IOP (mm Hg) |
|
13 |
10 |
|
26 |
20 |
|
52 |
40 |
|
78 |
60 |
|
104 |
80 |
Advantages: Prevents AC fluctuations and the sudden collapse of AC and its complications (choroidal detachment, expulsive hemorrhage, etc.) Esp. helpful in nucleus delivery (Positive pressure in AC pushes out the nucleus) and cortical wash (maintains AC, inflates the bag and makes it easier to visualize cortical matter)
Disadvantages:
- DM detachment at the site of entry may occur. Some amount of corneal hydration may occur around the site of entry of ACM making it difficult to visualize the 6 o’clock area
- Post-op leak in case of insufficient hydration after removing ACM
- PC rent, if occurs, extends and involves a large area of PC very rapidly in case the ACM is on.
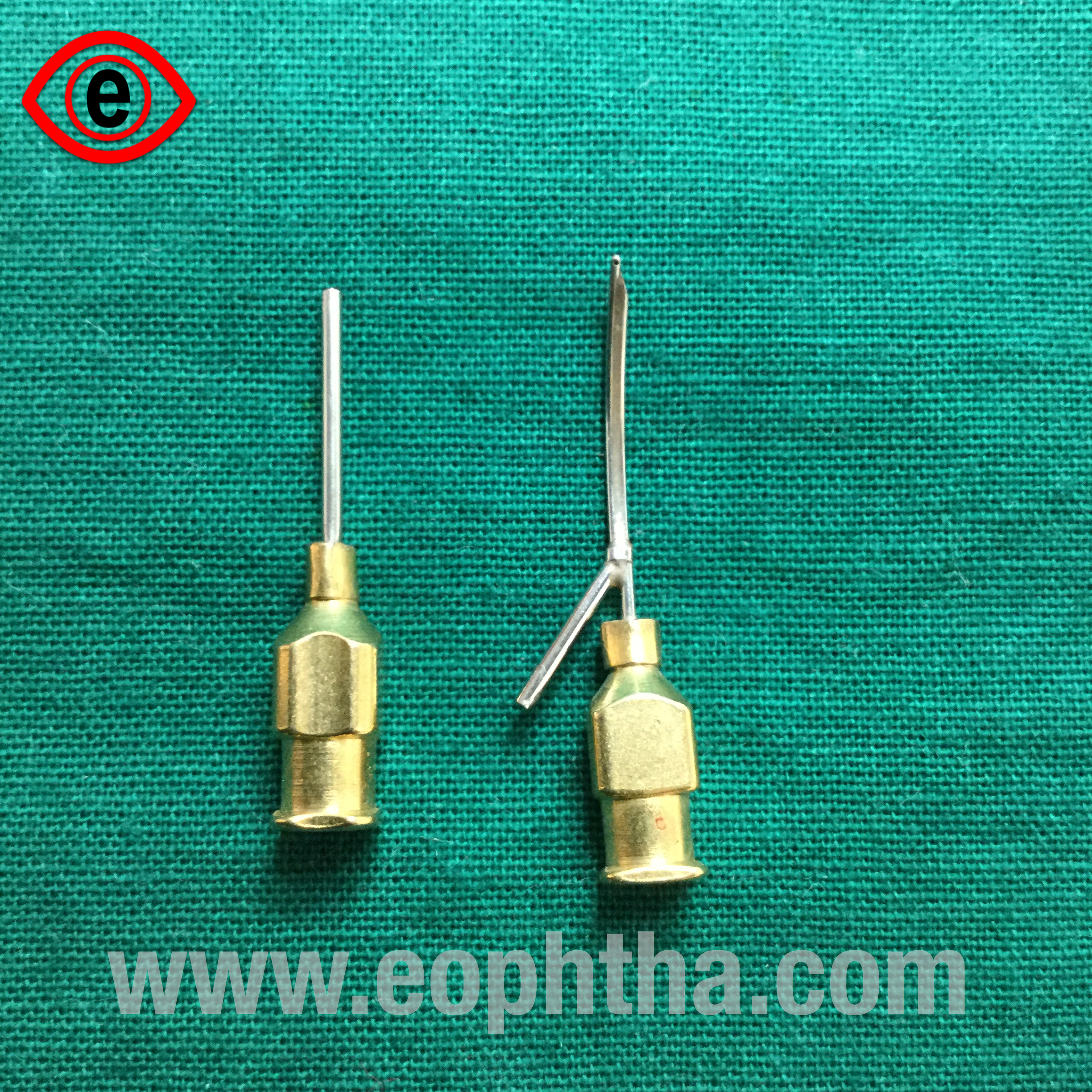
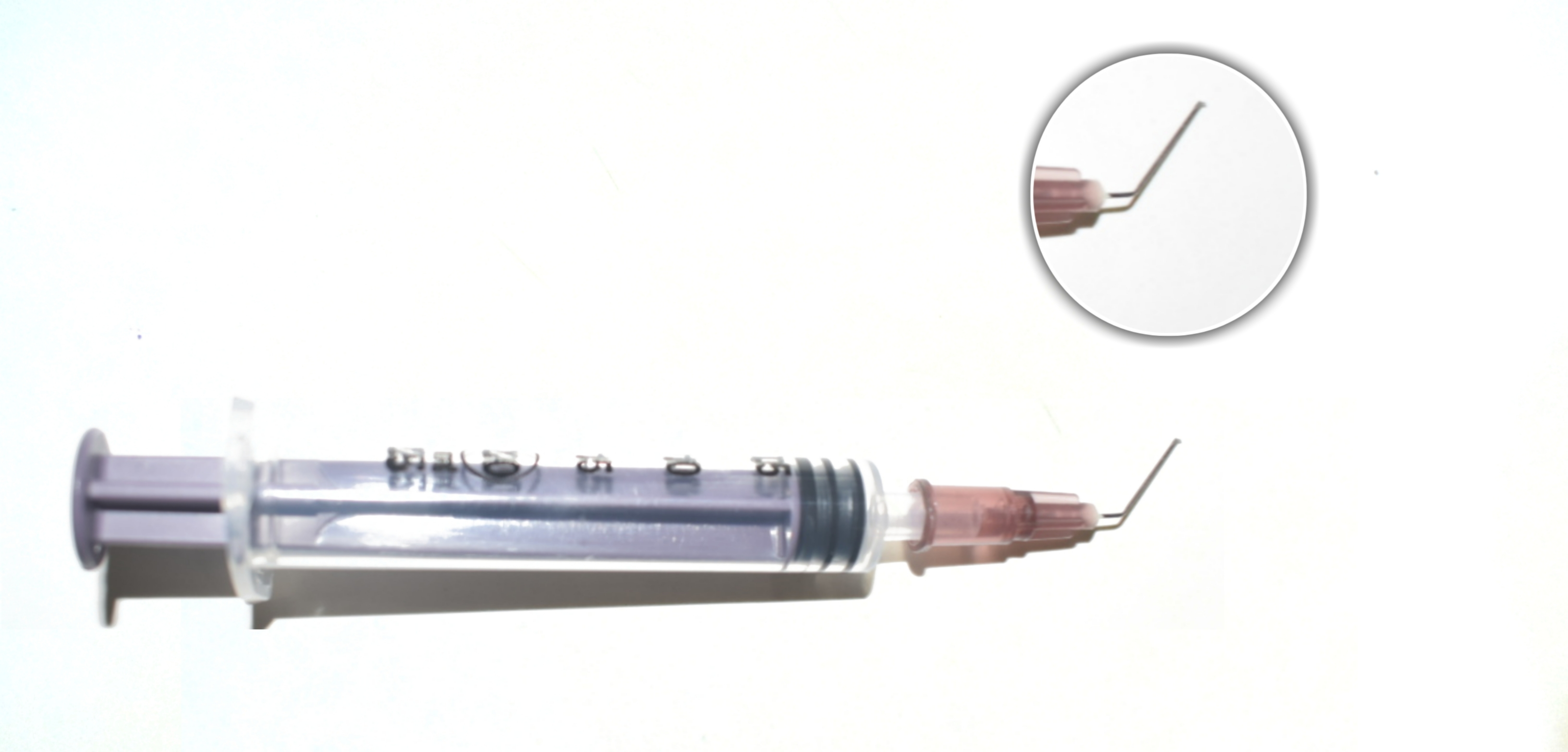
Single-port cannula:
Angulated tip
Better visualization of tip
23G
Uses:
For cortical wash/aspiration in case of SICS/ PE
Attached usually to a 5cc syringe
Enter via side-port/paracentesis to prevent AC collapse
Use your dominant to pull the piston of the syringe
PC polish
Advantages: Smooth tip- prevents damage to PC
Blumenthal cannula:
- Angulated tip (450)
- Sturdy
- 25 G
Uses:
- For hydrodissection in case of SICS
- Enter via paracentesis
- Signs of complete hydrodissection: AC shallows, Wave of fluid seen b/w lens and PC, Nucleus rotates freely
- Nucleus prolapsed into AC in case of SICS
- Enter via main entry/ tunnel
HydroCannula:
Instrument:
- Angled tip
- 27 G

Uses:
- To hydrate side-ports and ACM entries on completion of intraocular surgeries
- For hydro-dissection and hydro-delineation
Advantage
- Longer cannula easier to reach near the equator
- The golden ring is seen in hydro-delineation
- Nucleus prolapsed into AC in case of SICS
Castraveijo’s Caliper:
Instrument:
- Measuring scale at one end and pointed caliper tip at the other
- Spring action
- Has a screw 2 lock/fix the length measured
- Range: 0-20mm
Uses:
- To measure the diameter of cornea, as in buphthalmos, micro/megalocornea, etc.
- In various surgeries:
- SICS/PE: length of the incision
- Trabeculectomy: length of the scleral flap
- Squint: the amount of recession/resection of muscle
- Keratoplasty: occasionally used to determine the size of donor and recipient button
- RD surgery: to measure the distance for passing encircling band and to make ports at pars plana
- Ptosis surgery: measure the amount of LPS resected
- To measure the dimensions of a biopsy specimen
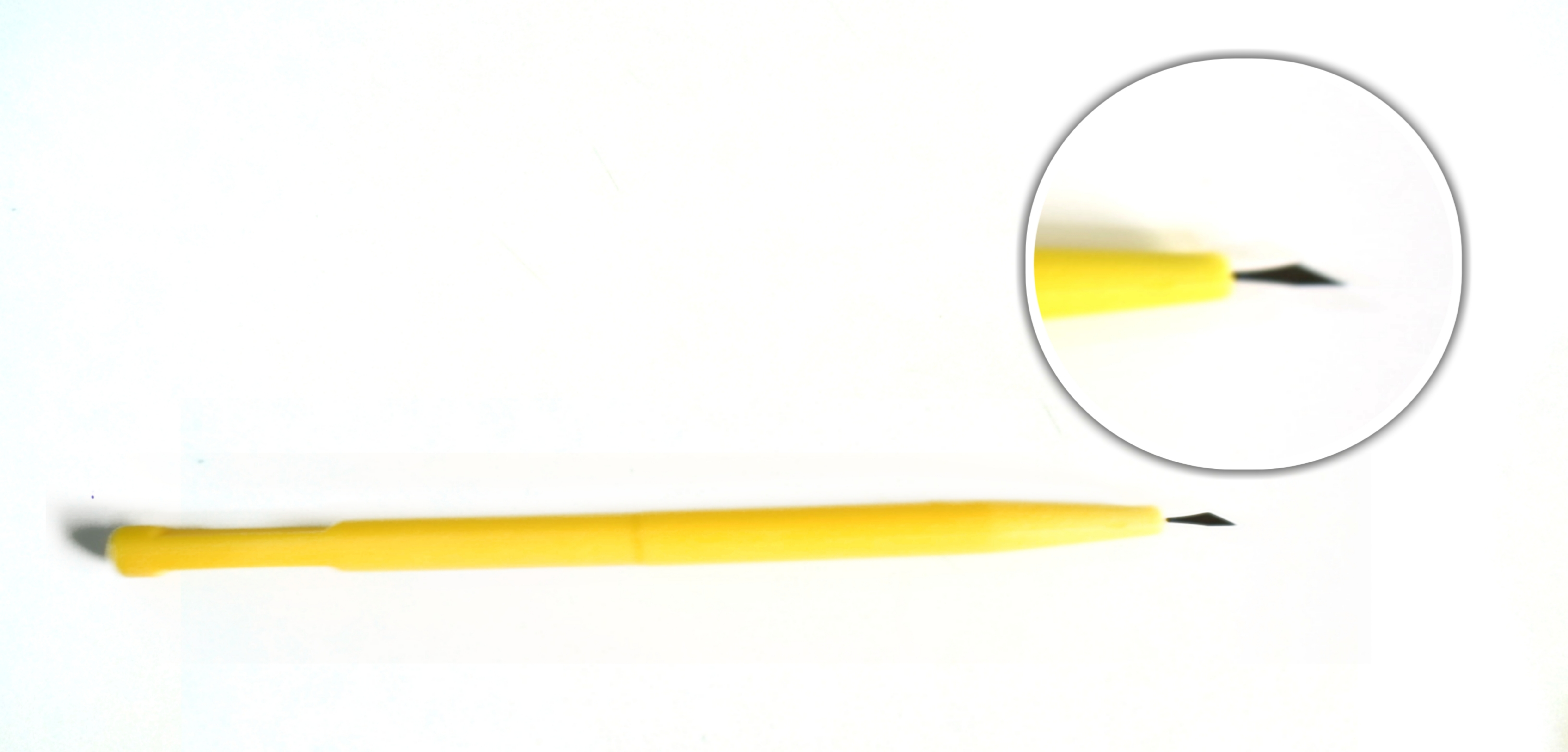
MVR blade:
Instrument:
- 20G
- Tip shaped like a spear
Uses:
- To create an entry/tunnel for ACM in SICS
- Usually made around 6 o’clock
- Ideal length: 1.5-2mm
- Enter at about 700 and then turn the tip parallel to iris plane once the tip is just seen to enter the AC
- Can be used to make side-ports too
- Sclerotomy ports in posterior segment surgeries
- To scratch ERM / ILM in VR surgeries
Crescent knife:
Instrument: Thin crescentic blade (usually bevel up) attached to a polycarbonate handle (450 angulation).Curved knife with cutting edges all around (front and sides) mounted on a disposable or reusable long handle.
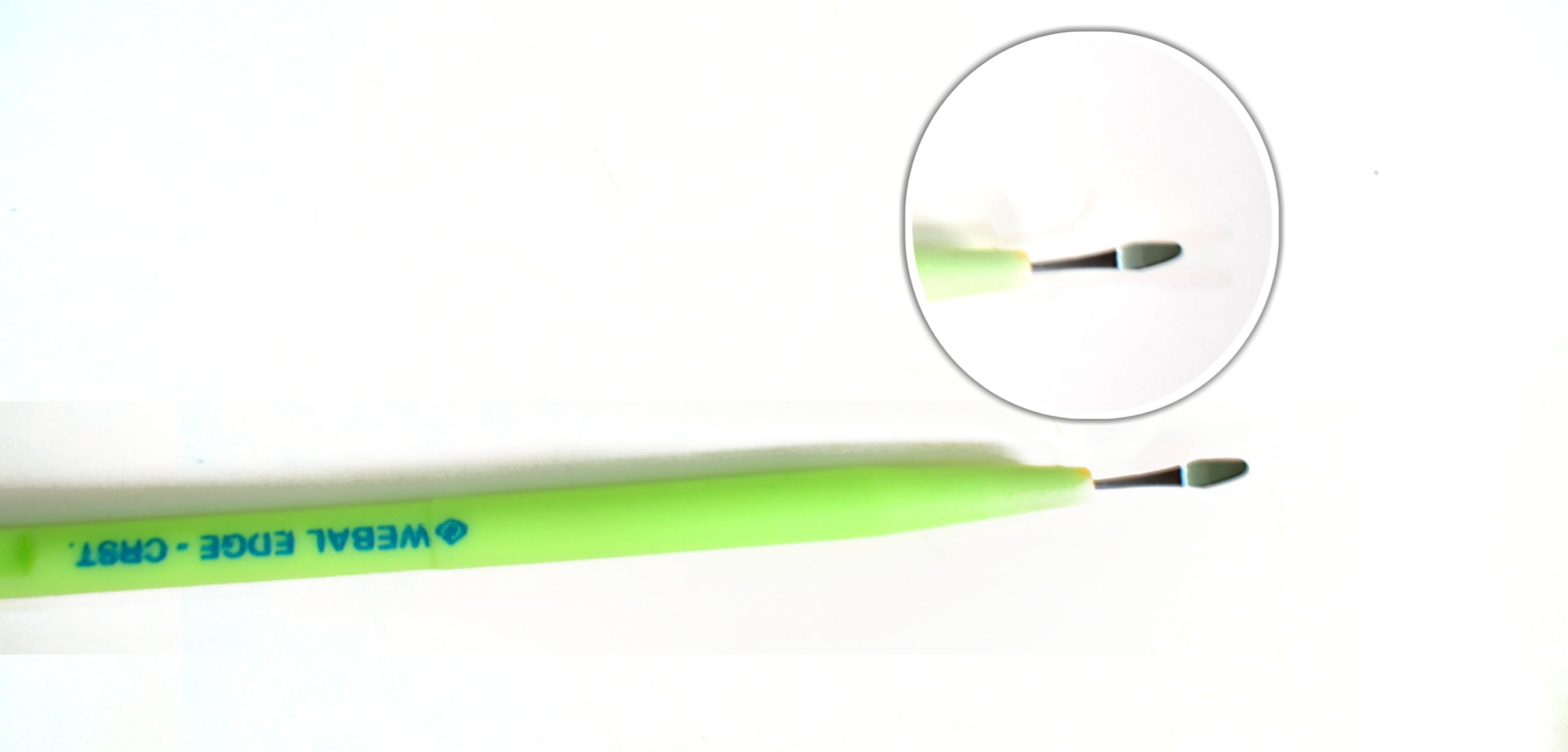
Uses:
Make sclera-corneal tunnel in SICS/PE
-
- Use wriggling movements
- Start from the centre ? complete one side and then go to the other
- Make a large inner lip (9-11mm dia)
- The smiling incision has the maximum flattening effect (ATR astigmatism)
Make sclera flap in trabeculectomy surgeries
Lamellar corneal dissection in lamellar corneal surgeries
15-degree blade:
Instrument:
- Thin straight blade (150) attached to a polycarbonate handle
- Maximum width passes a 20G instrument
Uses:
- To make side-port entries in various intraocular ant segment surgeries- Parallel to the iris plane
- For suture removal
- To make trabeculectomy scleral flap
- To enter AC while making stoma in trabeculectomy
- To make the palpebral conjunctival incision in I&C of chalazion
Wire vectis:
Instrument: A steel handle with a long tip ending in a loop (round/oval)
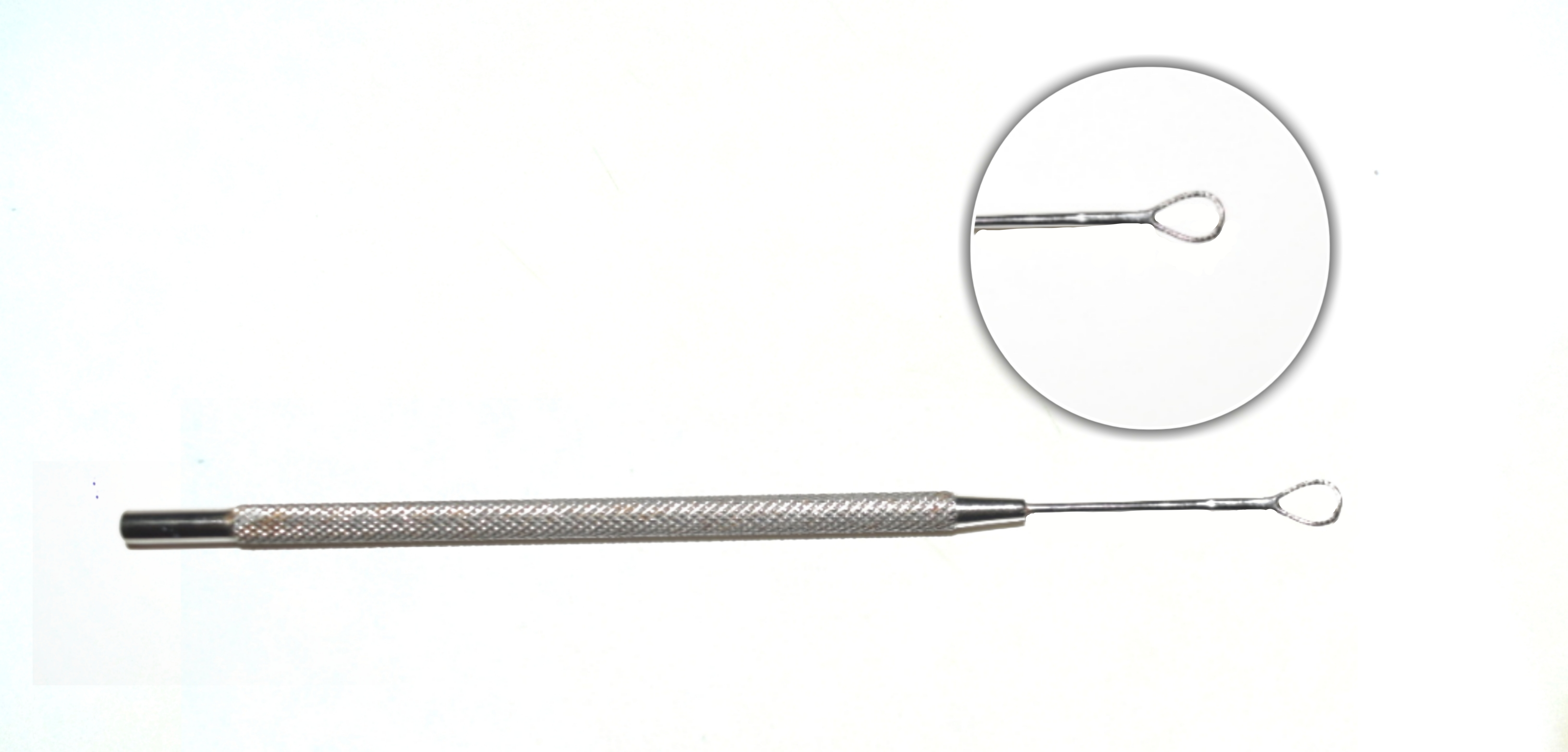
Uses:
- To remove the subluxated/ dislocated lens
- To deliver the nucleus in SICS/ECCE
- Ensure good papillary dilatation before introducing vectis
- Go b/w the lens and the PC and beyond the lens edge
- Be careful not to catch the pupil margin
- Lift up the lens and then withdraw
Disadvantages:
- Endothelial damage if the nucleus rubs against it while delivery
- Iridodialysis – if papillary margin caught b/w vectis loop and nucleus
- PC rent
- Sudden shallowing of AC
Irrigating vectis has 3-5 irrigating pores in the loop through which BSS/ irrigating fluid flows.
Advantages:
-
- Irrigating fluid creates hydrostatic pressure which along with the pull of the vectis helps deliver the nucleus out
- The fluid pushes the PC back and thus decreases the chances of PC rent.
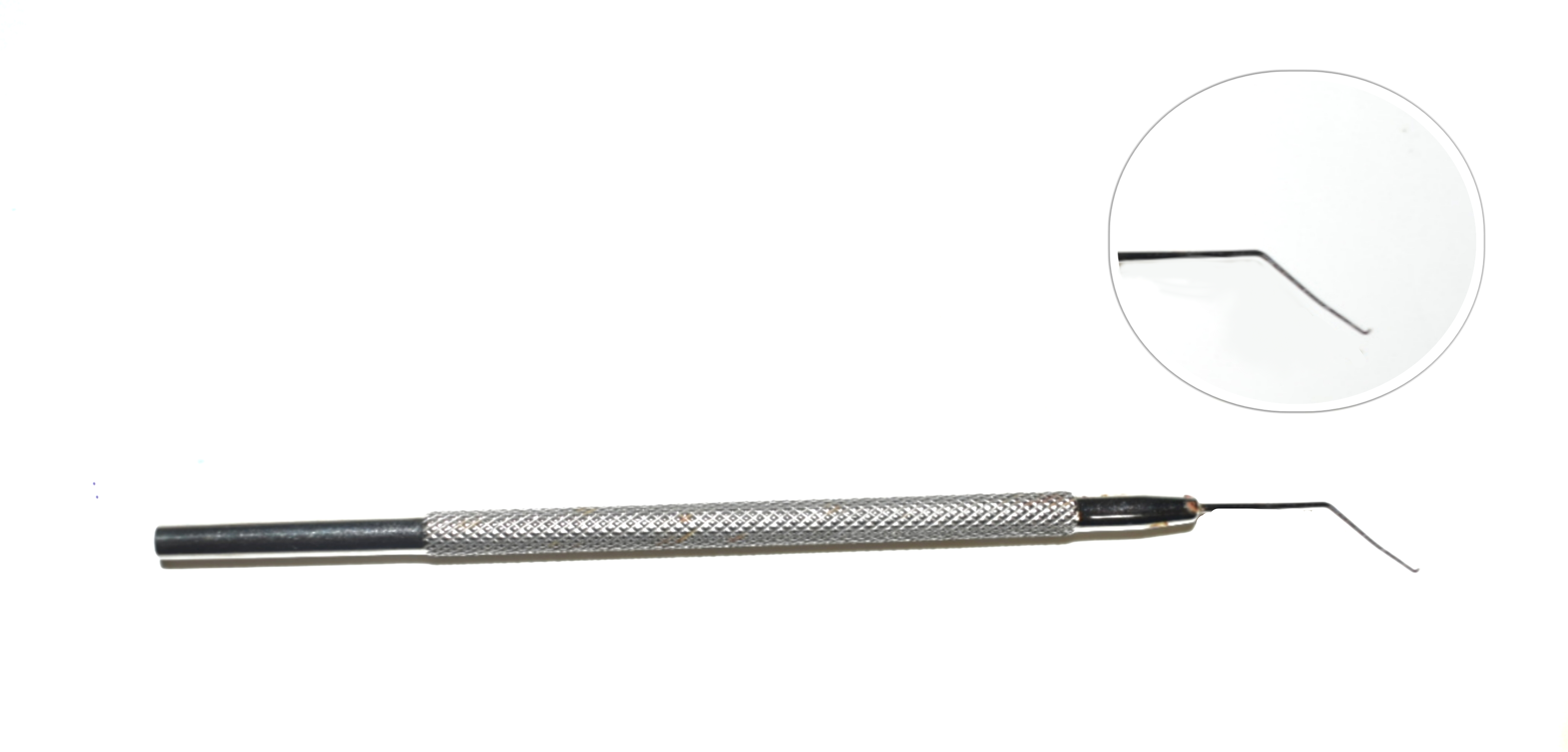
Cystitome or Capsulotome
Disposable cystitome is prepared by double bending the disposable 26 gauge or 30 gauge needles. One bend is at base and other at the tip of the needle.
Uses: It is used for doing anterior capsulotomy or capsulorhexis during cataract surgery.
IOL dialer
It is a fine but stout instrument with a bent tip. The tip engages the dialing holes of the IOL.
Uses: It is used to dial IOL for proper positioning in the capsular bag. It can also be used for other manipulations like nucleus rotation post hydrodissection, iris manipulations, etc.
Comments