


Entropion is the turning inward of the eyelid margin. Unlike ectropion, it is symptomatic and injures the ocular surface. The patient seeks medical care early.Ectropion is an eyelid malposition in which the eyelid margin does not oppose the globe.We shall discuss the relevant anatomy and clinical examination for the two entities together.
Relevant Anatomy
The eyelid can be grossly divided into
- Anterior lamella composed of skin and orbicularis
- Posterior lamella composed of tarsus and conjunctiva
Factors contributing to the stability of the lower eyelid
- Appropriate horizontal tension of the lower lid so that the eyelid is apposed to the eyeball. This is supplied by the medial and lateral canthal tendons.
- Lower lid retractors applying appropriate tension to the inferior margin of the tarsus, pulling the lower edge of the tarsus inferiorly, and thus preventing the lid margin from turning inward as in entropion, or outward as in ectropion.
- Synchronous movement of the inferior rectus and lower lid retractors so that the eyelid moves downward as the eye travels in downgaze
- A balance between the anterior and posterior lamellar tension.
Clinical Evaluation
We shall consider the examination of the patient keeping in mind the different etiologies of entropion and ectropion.
Slit Lamp Examination
Cornea: Look for Exposure keratopathy in paralytic entropion, superficial punctate keratopathy in entropion. Staining with fluorescein can help to identify changes. Superior pannus may be present in cicatricial entropion of trachomatous etiology. Limbal stem cell deficiency and conjunctivalization of the cornea can be present in cicatricial entropion resulting from Steven Johnson Syndrome.
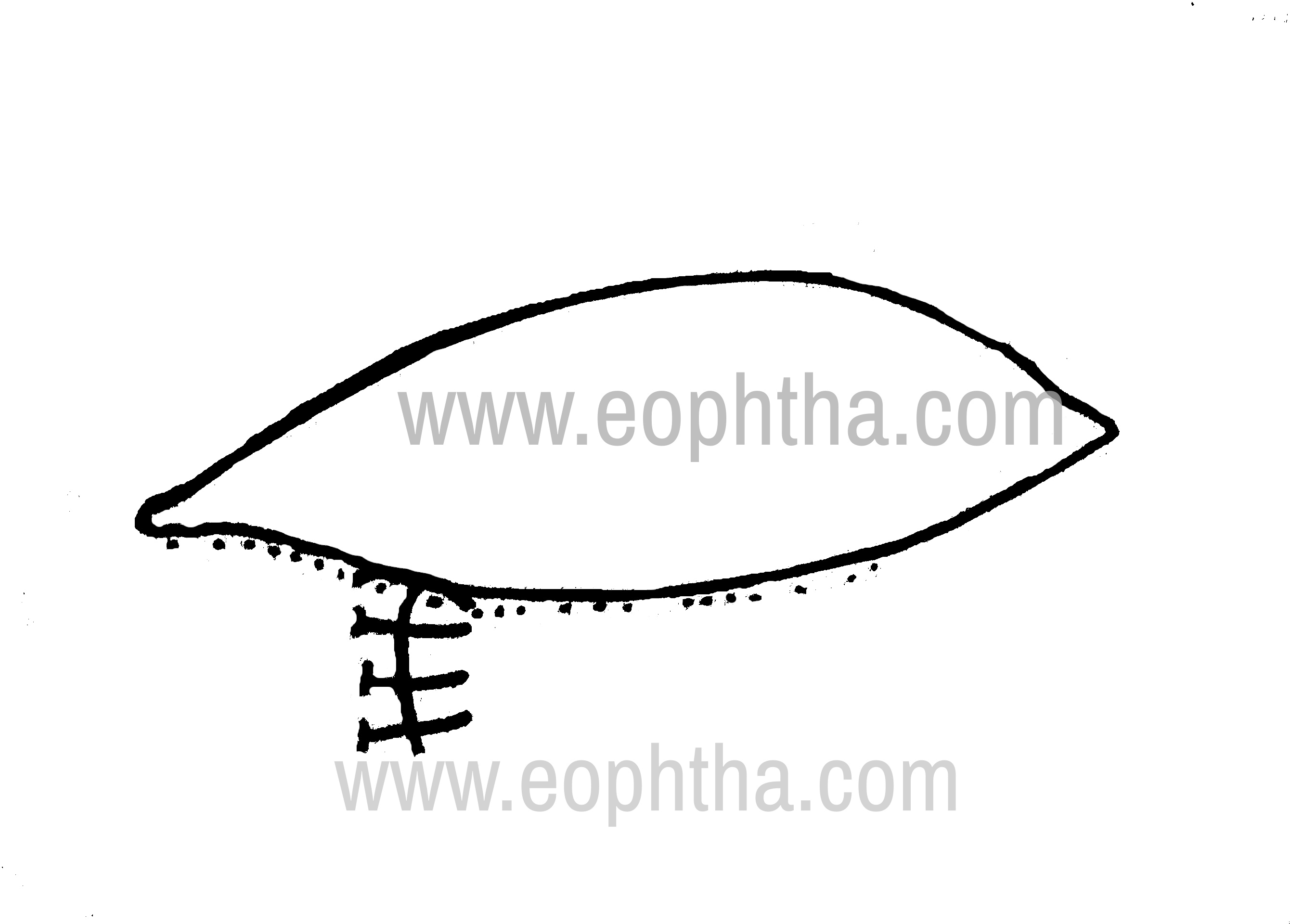
Conjunctiva: Congestion of conjunctiva may be present in chronic cicatrizing conjunctivitis, or in exposure keratopathy. Shortening of fornix and symblepharon formation may be early indicators of ocular cicatricial pemphigoid. Thickened tarsal plate, and horizontal linear scarring of upper tarsal conjunctiva (Arlt’s line) (Fig.1) may be present in trachomatous entropion.

Eyelid margin: The presenceof keratin along the eyelid margin indicates Steven Johnson Syndrome. If the punctum is visible without distracting the lower lid, that is an indication of punctal ectropion. Examination of the eyelid margin will differentiate entropion from trichiasis or distichiasis.
Eyelid Examination.
Horizontal eyelid laxity is evaluated by :
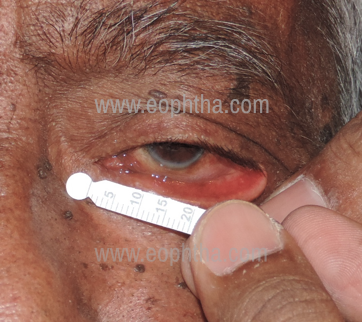
a. Eyelid distraction test: Manually pulling the eyelid away from the eyeball. Normally, lower eyelid should not move more than 6 mm off the eyeball (Fig.2).

Eyelid distraction test
b. Snap back test: Pulling the lower eyelid inferiorly toward the inferior orbital rim. Normally, eyelid will spring back into position without a blink. In moderate laxity, the eyelid will snap into position after a blink. If there is severe laxity, eyelid will remain away from the eye for a considerable period of time (Table 1)
|
Grade |
Criteria |
|
Normal |
Springs back immediately |
|
I |
2-3 sec |
|
II |
4-5 sec |
|
III |
>5 sec |
|
IV |
Does not resume normal position |
Table 1: Grading of snap test
Medial canthal tendon (MCT) laxity: Eyelid is pulled laterally and a lateral excursion of inferior punctum more than 2 mm denotes MCT laxity. (Figure 2b)
Medial Canthal Tandon Laxity
Lateral canthal tendon (LCT) laxity: Identified grossly by a rounded contour of the lateral canthus.(Figure 3) The lateral part of the eyelid is moved medially and displacement of the lateral canthus is noted. Displacement of more than 2 mm denotes LCT laxity.

Rounding of the lateral canthus
Laxity or disinsertion of lower lid retractorsPalpation just beneath the tarsus during vertical gaze shifts may reveal the disinserted edge of the capsule-palpebral fascia. In such cases, the conjunctival fornix may appear pink from the presence of orbicularis muscle instead of the retractor. Increased forniceal fat prolapse is usually noted in cases of retractor disinsertion.
The lower eyelid does not move down on downgaze. This called lid lag (not to be confused with lid lag in thyroid orbitopathy)
Assessment of anterior lamella: Any scarring of anterior lamella can be noted on inspection. A shortened anterior lamella will make the lower lid ectropion and retraction more prominent in an attempt to open the mouth. The lower lid in normal cases can be pulled up over the cornea; it cannot be pulled upwards in case of shortening.
Forniceal depth- Usually increased with retractor disinsertion and decreased with cicatricial conditions
Dynamic assessment: In the case of early senile entropion, the condition may be intermittent, hence not evident immediately. Asking the patient to forcefully close the eyes will cause rolling of pre-tarsal orbicularis over pre-septal orbicularis, and elicit the entropion.
Assessment of facial nerve weakness: Attempted closure of the eye will show lagophthalmos. Examination of facial symmetry will show loss of frontalis action, weakness of buccinator on the ipsilateral side, with a deviation of the angle of the mouth to the contralateral side.
Entropion
Kemp And Collin Grading of Entropion
- Minimal-Apparent posterior migration of meibomian glands. Conjunctivalization of eyelid margin + eyelash/globe contact on up gaze
- Moderate-Features of minimal entropion + eyelashes touching the globe in the primary position with or without thickening of the tarsal plate
- Severe-Gross eyelid distortion + metaplastic eyelashes + presence of keratin plaques + eyelid retraction causing incomplete trichiasis
Types
|
Congenital |
Acquired Involutional Cicatricial Spastic |
Congenital Entropion
Causes
Upper eyelid – due to mechanical effects secondary to micro-ophthalmos and enophthalmos
Lower eyelid – due to maldevelopment of inferior retractor aponeurosis
Tarsal Kink Syndrome is a type of congenital entropion that occurs with the deformity of the tarsal plate. It is a rare but severe form of entropion in which there is a fold or kink in the upper tarsal plate along its horizontal length leading to a corneal abrasion, ulceration, and amblyopia. The upper eyelid crease is typically absent on the affected side and the eyelid margin is turned inward.
Etiology of Tarsal Kink Syndrome
- primary tarsal defect
- direct mechanical pressure on the tarsus in utero
- disinsertion of the levator aponeurosis
- secondary blepharospasm from corneal abrasion
- overaction of the marginal fibers of the orbicularis muscle.
Surgical correction is urgent and the procedures described include direct excision of the kink, excision with posterior lamellar scleral graft, lamellar tarsoplasty , eyelid everting sutures, anterior lamellar repositioning, margin rotation, partial tarsotomy with levator repositioning, levator aponeurosis reattachment, and crease reformation, and inter-marginal suture tarsorrhaphy.
Involutional Entropion (Figure 4)

Involutional Entroption
Predisposing factors:
a. Horizontal eyelid laxity: due to stretching of the lateral canthal tendon
b. Vertical eyelid laxity due to weak lower eyelid retractor/disinsertion of lower eyelid retractors: Normally, they pull at the lower edge of tarsus inferiorly and posteriorly, thus preventing the inward turning of the eyelid margin. When lax, it allows the eyelid margin to invert
c. Overriding of pre-septal over pretarsal orbicularis muscle
Clues to overriding of preseptal over pretarsal orbicularis
- Rounded eyelid margin
- The occurrence of entropion on forceful eyelid closure
- Relative enophthalmos with deep superior sulcus
d. Involution of the soft tissues of the orbit, particularly the orbital fat, may lead to involutional enophthalmos, which in turn can lead to unstable eyelid position with entropion.
Spastic Entropion
It is usually predisposed in patients with redundancy or disinsertion of the lower eyelid retractor complex and those with horizontal eyelid laxity. It can be precipitated by intraocular surgeries.
Spastic closure of the eyelids → orbicularis oculi muscle overwhelms the opposing action of the lower eyelid retractor→in-turning of the eyelid
Cicatricial Entropion

Cicatricial Entropion
The pathophysiology of cicatricial entropion is as follows:
- Shortening of the posterior tarsoconjunctival lamella relative to the anterior lid surface.
- Shift in favor of the posterior vector of the normally balanced anterior and posterior forces
- Deformation of the tarsus
- In-turning of the eyelid margin (even in the absence of any significant horizontal or vertical eyelid laxity.)
When the eyelid is stretched laterally by the finger of the examiner, the involutional entropion gets rectified; the cicatricial entropion does not improve.
Causes
- Ocular cicatricial pemphigoid
- Steven-Johnson syndrome
- Linear IgA bullous dermatosis
- Allergic blepharoconjunctivitis
- Erythema multiforme
- Chemical burns
- Traumatic injuries
- Infectious (trachoma and herpes zoster)
- Topical medications (miotics, idoxuridine, timolol, pilocarpine, and dipivefrin).
Severe dry eyes due to loss of conjunctival goblet cells and accessory lacrimal glands may be associated with cicatricial entropion.
Treatment Of Entropion
Medical management is not curative. It is used to temporize in patients who may not be able to tolerate surgery or to those awaiting definitive surgical intervention.
- Topical lubrication- to help protect the cornea
- Taping the eyelid skin to the cheek or brow -to evert the lid margin
- Botulinum toxin- to weaken the orbicularis muscle and prevent override onto tarsus
Everting Sutures
Sutures are passed to correct the lamellar dissociation as follows
- transverse sutures prevent upward movement of pre-septal muscle
- everting sutures tighten the lower eyelid retractors and evert the eyelid.
Wies procedure
Transverse eyelid split + everting sutures – eyelid is split transversely to create fibrous tissue scar barrier which prevents the upward movement of pre-septal muscle. Everting sutures shorten the lower eyelid retractors.
Quickert procedure
Transverse eyelid split + everting sutures + horizontal eyelid shortening – lower eyelid retractors are mechanically tightened and double-armed sutures are passed full thickness through the eyelid, entering the conjunctiva posteriorly low in the fornix and exiting on the anterior surface of the eyelid just inferior to the eyelashes. Sutures are tied tightly to give a slight overcorrection, which is left to dissolve over 10 days, and scar tissue holds the retractors in place. The scar forms a barrier for the overriding pre-septal orbicularis.
Jones’ Procedure
Plication of lower eyelid retractors creates a barrier to the upward movement of pre-septal muscles.
Surgical Steps
- Local anaesthetic containing epinephrine is injected into the lower lid fornix and anteriorly under the skin after marking the sub-ciliary incision
- Sub-ciliary incision is made with no. 15 blade or Colorado microdissection needle through the skin
- Colorado microdissection needle (or Westcott scissors) is used to cut the orbicularis muscle. Usually the sub-ciliary incision is superior to the inferior edge of the tarsus.
- Sub-orbicularis dissection is done and continued inferiorly toward the inferior orbital rim
- Lower lid retractors are identified (preaponeurotic fat is the landmark )
- Lower lid retractors are dissected off the conjunctiva and advanced on to the tarsus and reattached to the inferior edge of the tarsus using three interrupted 4-0 non-absorbable sutures
- Tension in the sutures are titrated to achieve a slight overcorrection on table
- Sub-ciliary incision is closed with either continuous or interrupted sutures using 6-0 absorbable suture
If horizontal eyelid laxity is a significant finding, repair may be achieved with simple horizontal eyelid shortening, with a full-thickness wedge resection in the lateral third of the eyelid and primary layered closure.
More commonly a lateral tarsal strip (LTS) canthal reconstruction is used, often combined with other procedures
Treatment Of Cicatricial Entropion
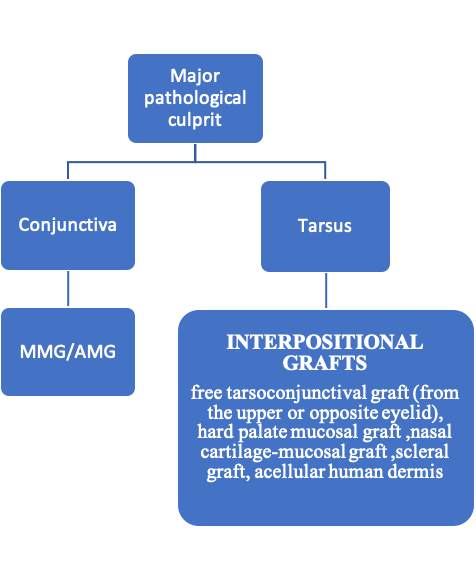
Management of cicatricial entropion should be deferred till the inciting factor is well controlled, and any active cicatrizing process is absent. The exception is a situation in acute chemical or other injuries, where the entropion has to be corrected to prevent compromise of the corneal surface. Cicatricial entropion is treated by lengthening of the posterior lamella.
a. Tarsal fracture operation/tarsotomy: This is indicated for mild cicatricial entropion of the lower lid and mild to moderate cicatricial entropion of the upper lid. The tarsal fracture operation lengthens and reorients the scarred posterior lamella minimally. A horizontal incision across the lower tarsus is made. The lid is then“fractured” or bent out. The surgical wound spreads apart. The wound is stabilized in an open position with double-armed 6-0 Vicryl sutures.
b. Posterior lamellar graft: This is indicated in moderate to severe cicatricial entropion after lysis of the scar tissue.
Treatment of Cicatricial Entropion
Treatment Of Spastic Entropion
- Eliminating the cause of underlying spasm
- Injection of a small dose of botulinum toxin into the pre-septal orbicularis oculi breaks the vicious cycle of muscle spasm and further irritation of the ocular surface by the eyelashes.
- Quickert suture as described earlier.
Ectropion
Ectropion one of the most frequently encountered eyelid malpositions in which the eyelid margin does not appose the globe. Its management and prognosis is subject to its etiology and site. Surgical approaches have been individualized and planned according to the preoperative assessment and a patient may require a single or combination of procedures based on the severity and mechanisms involved.
Mechanism:
Horizontal eyelid laxity as well as vertical foreshortening of the anterior lamella (skin and orbicularis muscle) play a role in development of ectropion. Hence, tightening of the lower lid as well as repositioning the lamellae to their normal anatomical positions is essential.
Etiology Of Ectropion
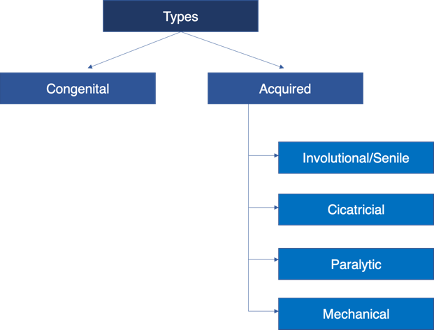
Congenital Ectropion:
- Blepharophimosis syndrome
- Microphthalmos
- Buphthalmos
- Orbital cyst
- Down syndrome
- Ichthyosis (Fig.7)
- Acute eversion: orbicularis spasm

Lamellar Icthyosis
Involutional Ectropion:
Pathophysiological consideration: horizontal lid laxity due to senile changes in orbicularis tone and laxity of canthi (Fig.8).

Involutional Ectropion
Those with an artificial eye may develop involutional changes due to constant rubbing and contact of the prosthesis with the eyelid, leading to stretching and disinserted capsulo-palpebral fascia.
Cicatricial Ectropion:
A scarred and vertically shortened anterior lamella can lead to outward turning of the eyelid due to an imbalance of forces. (Figure 9)

Cicatricial Ectropion
It can be present in the upper or lower lids.
- Trauma
- Burns
- Atopic dermatitis
- Iatrogenic (post- blepharoplasty, orbit surgery)
- Lamellar ichthyosis
- Basal cell carcinoma
- Drug-induced: Anti-glaucoma medications (eg. PG analogs, alpha-2 agonists), Anticancer drugs: eg. Docetaxel, erlotinib, cetuximab
Paralytic Ectropion (Figure 10)
This occurs secondary to varied causes of facial (VIIth) nerve palsy:
- Cerebellopontine angle tumors
- Herpes zoster oticus (Ramsay Hunt Syndrome)
- Parotid tumors

Paralytic Ectropion
Mechanical Ectropion: (Fig.11)
The weight of the lesions on the eyelid may overstretch the retractors, leading to the out-turning of the lid as a result of gravity, eg. Neurofibroma

Mechanical Ectropion
Management Of Ectropion:
Involutional Ectropion:
1. Retropunctal cautery
2. Medial spindle procedure: Tarsoconjunctival excision – lower punctum is everted and a diamond shaped area (6x3mm) of tarso conjunctiva is excised adjacent to the punctum and closed with absorbable sutures (Fig.12)
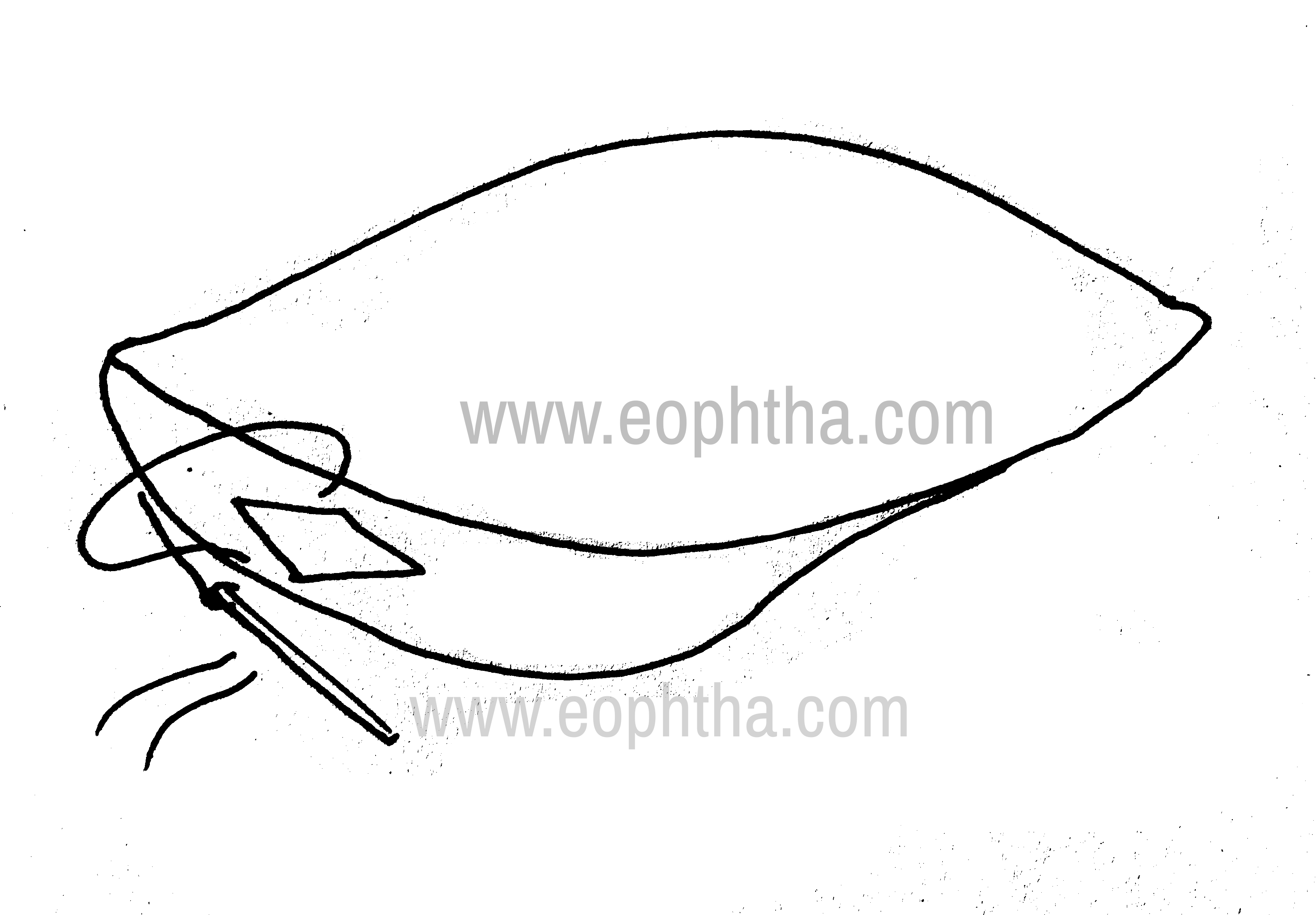
Medial Spindle Excision
3.Smith’s Lazy-T procedure: When medial ectropion is associated with horizontal lid laxity. Pentagonal wedge of eyelid tissue us resected 4mm lateral to the punctum. Conjunctiva is closed horizontally with interrupted absorbable sutures (Fig 13a,b)

Smith’s Lazy T procedure: excision
Smith’s Lazy T procedure: closure
4. MCT plicationLax MCT is sutured to the medial end of the lower tarsal plate
5. Pentagonal wedge resection:Generalized ectropion with horizontal lid laxity. Full-thickness pentagon is resected to correct excess horizontal lid laxity. Done at the area of maximum lid laxity (Fig.14a,b).

Pentagonal wedge resection: Excision

Pentagonal wedge resection: Closure
6. Smith’s modification of Kuhnt-Szymanowsky procedure:Done in the presence of excess horizontal laxity and the presence of extra skin. Through a subciliary incision, wedge resection is performed laterally. Excess skin-orbicularis layer is resected in the form of a base down triangular flap.
7. Lateral tarsal strip procedure:Done when there is co-existing LCT laxity. Lateral canthotomy is performed, the inferior crus of the tendon is incised. The tarsal strip is fashioned by scraping off mucosa from the lateral aspect. The strip is sutured to the lateral orbital tubercle.
Cicatricial Ectropion:
1. Medical management:
- Ocular lubricants
- Soft contact lenses
- Digital massage of scarred region with emollients
2. Local steroid or 5-fluorouracil injection into scar
3. Surgical management:
a. Z-plasty: done for vertical scars crossing skin tension lines. After excision of scar tissue, two flaps of skin are transposed to increase the length of the skin in the line of scar contraction
b. V-Y plasty: done for vertical scars with minimal shortening of skin. A ‘V’-shaped incision is made with the apex pointing to the base of the scar. The tissue is excised and the ‘V’ is closed in a ‘Y’ shape, lengthening the lid vertically.
c. Skin grafting: done in the presence of generalized skin shortage. Can be a transposition flap (monopedicle or bipedicle) from the upper lid or a full-thickness skin graft. A skin graft may be harvested from the upper lid, pre- or post-auricular, or medial forearm region. The skin once grafted should be scored for good drainage postoperatively. A traction suture placed for 1-week postoperatively will ensure lower chances of recurrence.
Paralytic Ectropion:
The primary aim is to protect the cornea.
1. Medical: lubricants, eye-patching
2. Surgical: when there is progressive corneal decompensation or anesthesia with poor Bell’s phenomenon
- Medial canthoplasty- for paralytic medial ectropion
- Lateral canthal sling
- Temporary suture tarsorrhaphy
- Fascial sling – when there is cheek ptosis as well (using fascia lata)
References:
1.Goldberg et al, Entropion repair. In Wobig JL, Dailey RA, eds, Oculofacial plastic surgery: face, lacrimal system, and orbit, pp. 91–97, New York: Thieme, 2004 2.Jonathan J. Dutton, Entropion.In A. J. Cohen, C. N. Burkat (eds.), Oculofacial, Orbital, and Lacrimal Surgery, pp.87-107, Switzerland: Springer Nature ,AG 2019 3.Beigi B, Kashkouli MB, Shaw A, Murthy R. Fornix fat prolapse as a sign for involutional entropion. Ophthalmology. 2008;115:1608–12. 4.Faria-E-Sousa SJ, de Paula Gomes Vieira M, Silva JV. Uncovering intermittent entropion. Clin Ophthalmol. 2013;7:385–8. 5.Naik MN, Honavar SG, Bhaduri A, Linberg JV. Congenital horizontal tarsal kink; a single-center experience with 6 cases. Ophthalmology. 2007;114:1564–8 6.Dutton JJ, Fowler AM. Botulinum toxin in ophthalmology. Surv Ophthalmol. 2007;52:13–31. 7.Winterhoff J, Köhler S, Laskawi R. Botulinum toxin for the treatment of spastic entropion. Case report. HNO. 2013;61:665–7. 8.Deka A, Saikia SP. Botulinum toxin for lower lid entropion correction. Orbit. 2011;30:40–2. 9.Swamy BN, Benger R, Taylor S. Cicatricial entropion repair with hard palate mucous membrane graft: surgical technique and outcomes. Clin Exp Ophthalmol. 2008;36:348–52. 10.Chen J, Wang Z, Gu J. Management of cicatricial entropion of the upper lid using acellular human dermal allograft. J Plast Reconstr Aesthet Surg. 2008;61:610–4 11. Collin J. A manual of systematic eyelid surgery. [Philadelphia, Pa.]: Butterworth Heinemann Elsevier; 2007. 12. AAO, Orbit, Eyelids, and Lacrimal System, 2018-19 13. Ing E. Ectropion: Background, Pathophysiology, Epidemiology [Internet]. Emedicine.medscape.com. 2018 [cited 24 June 2020]. Available from: https://emedicine.medscape.com/article/1212398-overview