


Introduction:
Anterior segment ocular imaging has gone through various inventions starting from the ultrasound in the 20th century to the recent AS- OCT.1 Ultrasound bio-microscopy, one of the ocular imaging devices is a high-resolution technique, which allows in vivo assessment of the structures of the anterior segment of the eye where cross-sectional images of ocular structures are obtained at microscopic resolution. 2The higher frequency of UBM ranging between 35 and 50 MHz, gives a depth of about 4 mm and an axial and lateral resolution of approximately 25 and 50 microns, respectively. 3 Being a non-invasive technique, efficient regardless of the clarity of the optical media and due to its portability can be performed both in adults and children with no complications.4 The internal acoustic characteristics of UBM, accompanied by the very fine backscatter speckle patterns, permit clear differentiation of ocular tissue at various levels.5 UBM imaging has been very useful in understanding the dynamics behind the mechanism of various ocular pathologies especially angle-closure glaucoma. This chapter discusses the various clinical applications of the UBM both in the diagnosis and management of ocular pathologies.
Background:
History of Ophthalmic Ultrasound:
Ophthalmic ultrasound for diagnostic imaging of the eye was initially attributed to the work of Mundt and Hughes (A-scan), Baum and Greenwood (B-scan) in the early 1950s. 6,7 Even though, there have been huge improvements in the development of technology since then, the centre frequency of ophthalmic ultrasound units has almost, remained at or near 10 MHz. 6 Although certainly useful for assessment of various ocular pathologies, the resolution obtainable at 10 MHz is poorer than that of current generation ophthalmic imaging devices like OCT. Hence ophthalmic ultrasound used initially was not useful in the diagnosis and management of anterior segment disorders especially glaucoma due to its poor resolution. To overcome this problem, UBM was invented which uses a frequency of 35- 50 MHz and hence better resolution.
History of UBM:
UBM was first introduced in the early 1990’s by theFoster and Pavlin group to overcome the difficulties due to an ultrasound B scan as described above. 8 Zeiss-Humphrey’s ultrasound microscopy was an outgrowth of the work by the Foster group. 9 The Zeiss-Humphrey UBM consisted of a 50 MHz probe which provided a scan rate of 8 Hz, giving real-time imaging, with scans consisting of 256 lines over a 5 mm × 5 mm field. 9 The Ultra link Artemis -2 UBM invented by the Coleman group, which is no longer in use emphasized the processing of raw radiofrequency echo data acquired in sequential planes suitable for 3-D analysis of the ocular structures.10 Recent versions of UBM produced by various groups including Optikon, Sonomed use higher scan rate and higher frequency (80 MHz by IScience) for higher resolution imaging of the angle.10
Mechanism of Acoustics and Ultrasound:
The image quality produced by the ultrasound is dependent on the three factors - frequency of the ultrasound, the length of the pulse and the ratio of the focal length to the transducer diameter (f-number) and.8 Higher frequency and shorter focal length are usually associated with higher resolution of the images but poorer penetration and hence the transducer is the critical component for proper image resolution. The transducer is moved linearly over a 5 * 5 mm image field in the current generation UBM devices, which generates sonographic data along each of 512 lines and the signal produced is amplified in proportion to the depth from which it originated using so called ‘time-gain compensation’. 8
The measurement accuracy of the imaging system is dependent on the following 4 factors - the stability of mechanical motion, lateral resolution, axial resolution, and the pixel size of the image. 8The lateral resolution depends on the distribution of ultrasound in the field of the transducer, which has a width at half maximum given by the product of the wavelength and the f-number. The axial resolution depends on the speed of sound in the various tissues and determined by ‘Instrument axial resolution’ and ‘measurement precision’.8 The following table demonstrates the differences between convention USG B scan and UBM (Table 1)
|
PARAMETER |
UBM |
ULTRASOUND B SCAN |
|
Frequency |
50 MHz |
10 MHz |
|
Axial resolution |
30 |
150 |
|
Lateral resolution |
60 |
450 |
|
F ratio |
2 |
3 |
UBM Technique and Interpretation:
Currently, there are two techniques for performing UBM – The immersionshell technique and the clear scan method without using scleral shell.11 In the latter technique, the patient can sit upright without going for the supine position. The UBM examination technique is almost similar to B-mode ultrasound where the transducer direction and manipulation of the probe is guided by looking at the image on the screen, the major difference being finer movements are required for performing UBM. The patient is examined in a supine position facing the ceiling for the immersion scleral shell technique. (Figure 1) After applying topical anesthetic drops, a specially-designed eyecup of 22 to 24 mm diameter (scleral shell) is used to separate the eyelids and filled with a viscous, sonolucent coupling fluid such as methylcellulose (1-2.5%). The images are stored in an electronic format on a computer attached to the device and the derivation of measurements from the images has to be done on the UBM’s computer unit or a PC which uses specific software to process and display the images.8

UBM Instrumentation:
The main parts of a conventional ultrasound biomicroscopy machine are
- Transducer – The main probe can be either handheld (Figure 2) or mounted on an articulate arm connected to the main unit (As pointed in figure 3)
- Computer with the main processing unit which acquires real-time images (Figure 3)

with arrows showing the –
computer with main unit,
articulate arm and the transducer
attached to the articulate arm
Angle Parameters in UBM:
The following quantitative angle parameters were proposed by Pavlin et al for quantitative measurement of angle recess and its subsequent use in angle-closure management.8
1. AOD - Distance between the trabecular meshwork and the iris at 500 microns anterior to the scleral spur
2. TCPD - Distance between the trabecular meshwork and the ciliary process at 500 microns anterior to the scleral spur
3. IT1 - Iris thickness at 500 microns anterior to the scleral spur
4. IT2 - Iris thickness at 2 mm from the iris root
5. IT3 - Maximum iris thickness near the pupil margin
6. ICPD - Distance between the iris and ciliary process along the line of TCPD
7. ILCD- Contact between the iris and the lens
8. TIAθ1 - Angle of the angle recess
Clinical Applications:
Sclera
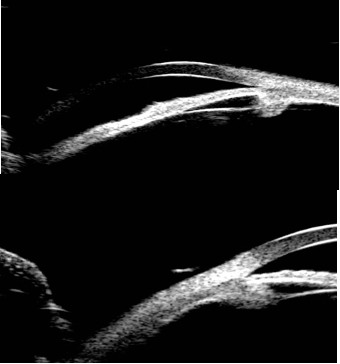
UBM is only able to examine the area of the sclera anterior to the equator due to the area limited by the scleral shell. 8 Typical UBM feature of the sclera is a regular high reflectivity signal with relatively lower reflective tissue surrounding or inside. It is commonly used to differentiate structural abnormalities of the sclera or episcleral tissues like ciliary staphyloma. It is also useful for the assessment of treatment outcomes of scleritis especially the reduction of inflammation and measuring the thickness of sclera with immunosuppressive agents.8
Cornea
UBM can differentiate the cross-sectional structure of cornea where except for the Descemet’s membrane and the endothelium all the other 3 layers can be differentiated by the reflectivity. 8,9 Hence UBM has been used to quantitative measurement of corneal edema, Descemet’s membrane detachment, qualitative measurement of corneal dystrophy, and various other pathologies. Pavlin et al. were the first to describe UBM imaging of the cornea.8, 9 Before the advent of AS-OCT, UBM can be used to measure scar depth, which may be a significant factor in patient management for choosing the type of surgery and candidate selection in refractive corneal surgery. 9 For measuring corneal thickness, compared to conventional pachymeters, UBM has the advantage of allowing imaging and biometry of 2-D corneal cross-sections instead of at individual positions thus giving a more precise measurement of corneal thickness.12
UBM has been used for assessment of the cornea following excimer laser photo keratectomy and various other refractive procedures. Allemann et al. used the Artemis-2 prototype UBM to quantify scar density which uses 3D generation of echo images. 13 Reinstein et al. modified this system by using an arc- scanner to image the full width of the cornea following laser in situ keratomileuses and demonstrated visualization of the flap, measurement of residual stromal thickness and epithelial compensation for curvature changes induced by ablation of underlying stromal tissue.14 Reinstein et al, also used the same technique for quantifying changes in early keratoconus patients and demonstrated significant parameters for screening purposes.15
Glaucoma:
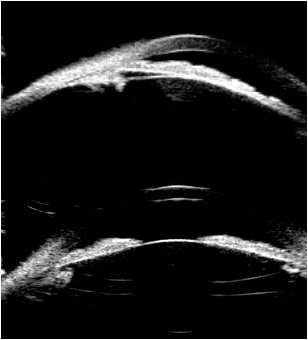
The main clinical application of UBM involves the opening of the anterior chamber angle and its subsequent value in the clinical management of angle-closure glaucoma. Pavlin et al. showed the utility of UBM in characterizing several forms of glaucoma, including plateau iris syndrome, pupillary block, secondary angle closure in pseudophakic eyes, and various other forms of angle-closure glaucoma.16
Pupillary Block: In pupillary block, forward bowing of the iris from the root to the pupil margin in the presence of a formed posterior chamber due to pressure difference between anterior and posterior chamber. Laser iridotomy will result in flattening of the iris, by relieving the anterior/posterior chamber pressure differential. UBM will demonstrate little iris bowing, but rather anterior positioning of the ciliary body and closing of the sulcus. It can clearly differentiate whether the pupillary block is related to lens-related factors or angle related factors.8
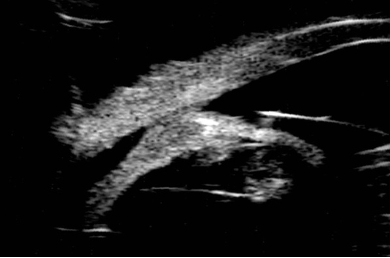
Plateau Iris Syndrome: In plateau iris syndrome, the UBM plays a most important role by allowing demonstration of anterior displacement of the ciliary processes and sulcus closure.8 UBM can also be useful for diagnostic imaging of aqueous misdirection syndrome, which is characterized by a flattened anterior chamber, typically following glaucoma surgery.8
Secondary Angle Closure in Pseudophakic Eyes: UBM has also been shown to be of value in elucidating the etiology of pseudophakic pupillary block glaucoma. Pavlin et al demonstrated the findings of pigment dispersion glaucoma with iris concavity, consistent with the hypothesis that iris-lens chafing is responsible for the dispersion of pigment particles. 17
Ciliary Body Effusion Syndrome: Ciliary body effusion secondary to drugs can be demonstrated by anterior rotation of the ciliary body, cystic spaces in the ciliary body, and surrounding sclera by UBM. It also plays a role in the management of the condition by doing serial UBM after withdrawing the offending drugs.8, 9
Glaucoma Surgery:
Peripheral Iridotomy and Iridoplasty Peripheral iridotomy remains the cornerstone of the management of angle-closure secondary to pupillary block which results in a significant increase in the angle width by eradicating the pupil block mechanism. UBM is a valuable tool in measuring the angle width pre and post laser iridotomy and Iridoplasty.8, 9
Cyclophotocoagulation Laser Cyclophotocoagulation, a cyclodestructive procedure for refractory glaucoma patients who have failed trabeculectomy or tube shunt procedure, or patients with minimal useful vision and uncontrolled IOP, or those being reluctant for surgery. It is done by two methods – trans-scleral and endo Cyclophotocoagulation. Accurate positioning of the laser probe is challenging in the destructive eyes and complications UBM is useful in the observation of postoperative changes and identification of postoperative complications.8, 9
Trabeculectomy It is one of the most widely performed glaucoma surgery procedures for glaucoma. UBM allows visualizing the status of surgical openings, outflow channel, and filtering bleb and useful for identifying the causes of operation failure.8, 9, 18
Uveitis Intermediate uveitis is an insidious type of uveitis characterized by inflammatory cells in the anterior vitreous, inferior pars plana. Because it can be seen by routine examination, the patients are often presented as secondary cataract, iris synechiae, vitreous floaters and cystoid macular edema. UBM is able to detect these changes and therefore able to provide further evidence for the diagnosis. 8, 9 Reduction in the number of ciliary processes and ciliary body detachment due to membrane traction plays a key role in the management of complications secondary to pars planitis especially hypotony.8, 9
UBM vs AS-OCT
AS-OCT is a newly evolved technique, used for imaging of anterior segment of the eye. Compared to AS-OCT, the main strength of UBM is its ability to visualize structures behind the iris, including the ciliary body and lens. 19 However, disadvantages compared to AS-OCT include the need for a water-bath immersion with direct contact to the eye which was overcome by the latest clear scan technique, longer image acquisition times, and the need for an experienced operator. Even though for certain form of glaucoma like ciliary body effusion, aqueous misdirection syndrome, UBM still remains the standard diagnostic tool, AS-OCT has its own advantages in angle-closure glaucoma as well. 19 However, for anterior segment tumours, AS-OCT offers clear-cut advantage over UBM.
The following table demonstrates the differences between UBM and AS-OCT (Table 2)
|
PARAMETER |
UBM |
AS-OCT |
|
Learning curve |
Requires a skilled operator Long learning curve |
Easy to operate Short learning curve |
|
Axial resolution |
Low |
High |
|
Depth of resolution |
High Can visualize structures beyond iris pigment epithelium |
Low Limited visualization of structures posterior to iris pigment epithelium |
|
Field of view |
Small |
wide |
|
Image acquisition time |
Slow |
fast |
In Ocular surface squamous neoplasia, AS-OCT shows a clear advantage by showing intralesional details and providing useful diagnostic information for management and follow-up. Conversely, in non-pigmented iris tumors, UBM was superior in identifying the posterior border of lesions with higher reproducibility compared to AS-OCT. 19, 20 Despite having a limited field of view and depth of visualization due to shadowing from keratinized and pigmented lesions, AS-OCT can be a reliable alternative in selected tumors since it is a fast, non-invasive and non-contact imaging technique. Despite the advantages of both UBM and AS-OCT imaging in anterior segment tumors, none of them is a substitution for biopsy, which still remains the gold standard for the diagnosis of ocular surface tumors.
Conclusion
UBM is an excellent tool for anterior segment imaging and in the diagnosis of various ocular pathologies. Despite the advent of newer imaging modalities like AS-OCT, UBM still has a role in the management of certain disorders due to its axial and lateral resolution and depth of penetration.
References:
- Ishikawa H. Anterior segment imaging for glaucoma: OCT or UBM?. Br J Ophthalmol. 2007;91(11):1420-1421. doi:10.1136/bjo.2007.121038
- Pavlin CJ, Foster FS. Ultrasound biomicroscopy of the eye. New York: Springer & Verlag; 1995.
- Pavlin CJ, Haraseiwicz K, Sherar MD, Foster FS. Clinical use of ultrasound biomicroscopy. Ophthalmology. 1991;98(3):287–295.
- Ishikawa H, Schuman JS. Anterior segment imaging: ultrasound biomicroscopy. Ophthalmol Clin North Am. 2004;17(1):7–20.
- Mannino G, Papale A, De Bella F. Biomicroscopia ad ultrasuoni [Ultrasound biomicroscopy]. Fabiano Editore; 2004. Italian.
- Mundt GH, Hughes WF. Ultrasonics in ocular diagnosis. Am J Ophthalmol 1956;42:488–98. [PubMed:13362453]
- Baum G, Greenwood I. The application of ultrasonic locating techniques to ophthalmology. II. Ultrasonic slit-lamp in the ultrasonic visualization of soft tissues. Arch Ophthalmol 1958;60:263–79.
- Overview of Ultrasound Biomicroscopy.Mingguang He, Dandan Wang, Yuzheng Jiang. Journal of Current Glaucoma Practice, January-April 2012;6(1):25-53
- Reinstein DZ, Silverman RH, Coleman DJ. High-frequency ultrasound measurement of the thickness of the corneal epithelium. Refract Corn Surg 1993;9:385–7.
- High-resolution ultrasound imaging of the eye – a review. Ronald H Silverman, PhD. Clin Experiment Ophthalmol. 2009 January ; 37(1): 54–67.
- Ama Sadaka, Prager T, Beaver H, Malik A. A novel use of ultrasound biomicroscopy. Eye (Lond). 2018;32(2):474-475. doi:10.1038/eye.2017.190
- Greyrose SE, Starr CE, Lloyd HO, Silverman RH. Comparative central corneal thickness by ultrasound pachymetry, Artemis-2, and Visante. IOVS 2008;49 ARVO E-Abstract 1020.
- Allemann N, Chamon W, Silverman RH, et al. High-frequency ultrasound quantitative analyses of corneal scarring following excimer laser keratectomy. Arch Ophthalmol 1993;111:968–73.[PubMed: 8328940]
- Reinstein DZ, Silverman RH, Coleman DJ. Very high-frequency ultrasound corneal analysis identifies anatomic correlates of optical complications of lamellar refractive surgery. Ophthalmology.1999;105:474–82. [PubMed: 10080202]
- Reinstein, DZ.; Archer, T.; Gobbe, M. Stability of LASIK in corneas with forme fruste or suspect keratoconus, where keratoconus was excluded by epithelial thickness mapping. American Academy of Ophthalmology Annual Meeting; 9 Nov 2008; Atlanta, GA.
- Pavlin CJ, Harasiewicz K, Foster FS. Ultrasound biomicroscopy of anterior segment structures in normal and glaucomatous eyes. Am J Ophthalmol 1992;113:381–9.
- Pavlin CJ, Macken P, Trope GE, et al. Accommodation and iridotomy in the pigment dispersion syndrome. Ophthalmic Surg Lasers 1996;27:113–20.
- Yamamoto T, Sakuma T, Kitakawa Y. An ultrasound biomicroscopic study of filtering blebs after mitomycin C trabeculectomy. Ophthalmology 1995;102:1770–76
- Huang D, Swanson EA, Lin CP, et al. Optical coherence tomography. Science. 1991;254:1178-1181.
- Janssens K, Mertens M, Lauwers N, de Keizer RJ, Mathysen DG, De Groot V. To Study and Determine the Role of Anterior Segment Optical Coherence Tomography and Ultrasound Biomicroscopy in Corneal and Conjunctival Tumors. J Ophthalmol. 2016;2016: 1048760.