
Introduction
The optic nerve consists of approximately 1.2 million axons that arise from the retinal ganglion cells and acquire myelin sheath proximal to lamina cribrosa. These axons do not have the capacity to regenerate. The normal optic disc is pink in color due to the fact that light entering the optic disc is conducted along the transparent nerve fibers and they diffuse among columns of glial tissue and capillaries. When axons are damaged in optic atrophy, light is reflected from opaque glial cells and does not pass through the capillaries. In addition, the reduced capillary vascularity and loss of tissue causes visibility of opaque scleral lamina cause the disc to appear pale.
Optic atrophy is the sequelae of progressive optic nerve disease that causes irreversible damage of ganglion cells and the retinogeniculate pathway. This degeneration along with gross reduction in capillaries results in loss of optic pathway conduction and pallor. Exploring the etiology of optic atrophy may lead to unexpected surprises as it may be the initial presentation of various neurological or systemic diseases at times . Pallor usually signifies that optic neuropathy has occurred a minimum of 2-3 weeks earlier 1
Optic disc pallor can be due to previous unidentified causes like ischemic optic neuropathy, trauma, optic neuritis, or several other forms of optic neuropathy. However, it is prudent to evaluate all patients with optic atrophy in order to identify a treatable cause of optic nerve pathology. Management of optic disc pallor requires a detailed history taking, stepwise anterior and posterior segment ocular evaluation, and careful optic nerve function assessment. Referral neurological examination and apt neuroimaging of brain - mostly preferred is MRI brain and orbit, has to be done.
Classification of optic atrophy2,3
Several methods have been proposed to classify optic atrophy and for the purpose of understanding, we can categorize them into
- Pathological
- Ophthalmoscopic
- Etiological
Table 1. Pathological optic atrophy
|
Ascending |
Descending |
Trans synaptic (transneuronal degeneration) |
|
The primary lesion is in the retina, optic nerve, or choroid, and the atrophy proceeds towards the brain. It is otherwise known as Wallerian degeneration |
The primary lesion is intracranial and it proceeds towards the optic nerve. |
A phenomenon by which neurons on one side of the synapse degenerates as a consequence of loss of neurons on the other side. It can be in congenital or acquired retinogeniculate lesions |
Table 2. Ophthalmoscopically - optic atrophy can be classified into five types
|
Primary |
It occurs when there is degeneration of optic nerve fibers and replacement by glial tissue.It occurs in an orderly manner without any alteration in the architecture of the optic nerve head |
|
Secondary |
It occurs when the architecture of the optic nerve head is lost due to degeneration of optic nerve fibers along with the excessive proliferation of glial tissue.this usually follows a optic disc swelling |
|
Consecutive |
It is associated with diseases of retinal vasculature, retinal ganglion cells, and choroid, and hence changes in the surrounding retina are commonly seen |
|
Cavernous |
There is axonal degeneration without any proliferation of glial tissue and characteristic formation of caverns which are filled with hyaluronic acid resulting in excavation of optic disc typically seen in glaucomatous optic atrophy |
|
Sectoral or partial optic atrophy |
It can be temporal or altitudinal disc pallor. Temporal pallor results due to involvement of the papillomacular bundle and commonly seen in toxic, nutritional optic neuropathy. NAION initially presents with disc swelling followed by sectoral disc pallor. |
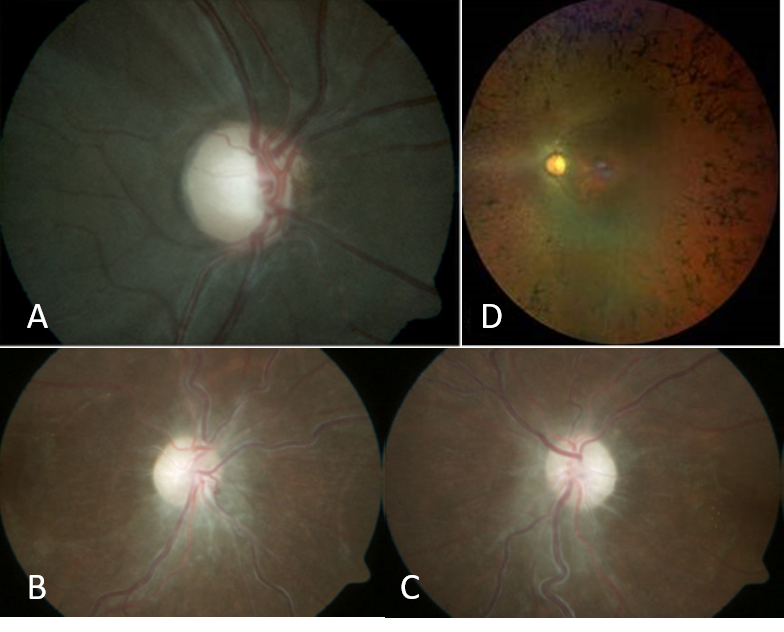
Figure 1: A. Primary Optic Atrophy B & C. Secondary Optic Atrophy D. Consecutive Optic Atrophy
|
Primary |
Secondary |
Consecutive |
Cavernous |
Segmental or partial optic atrophy |
|
|
Disc appearance |
Chalky white in color |
Dirty grey in color |
Waxy pale |
Vertically enlarged cup,with many lacunae, Notching of neuroretinal rim |
Pallor seen temporally or it can be sectoral |
|
Disc margin |
Well defined |
Ill-defined |
Normal disc margin |
Well defined |
Well defined |
|
Lamina cribrosa |
Lamina cribrosa is seen |
The physiological cup is obliterated and filled with glial tissue obscuring the view of lamina cribrosa |
Normal physiological cup |
Laminar dot sign,backward bowing of lamina cribrosa |
|
|
Retina and blood vessels |
Retinal vessels and surrounding retina are normal |
Peripapillary sheathing of retinal arteries |
Marked arteriolar attenuation, Associated retinal pathology is seen |
Baring of circumlinear vessels, Bayonetting and nasalization of retinal vessels, Nerve fiber layer defects |
Blood vessels and surrounding retina are normal |
|
Examples |
Optic neuritis, compression by intracranial tumors aneurysm trauma Hereditary optic neuropathy |
Post papillitis, Post papilledema |
Retinitis pigmentosa, choroiditis, myopia, extensive pan-retinal photocoagulation, Central retinal artery occlusion |
Glaucomatous optic neuropathy |
Nutritional and toxic optic neuropathies (temporal) Anterior ischemic optic neuropathy (altitudinal) |
Table 3. Fundus features in different types of optic atrophy
|
Post-inflammatory/post-infective |
|
Trauma |
|
Toxic |
|
Metabolic |
|
Circulatory/ischemic |
|
Consecutive |
|
Pressure and traction |
|
Hereditary |
Table 4. Etiological classification
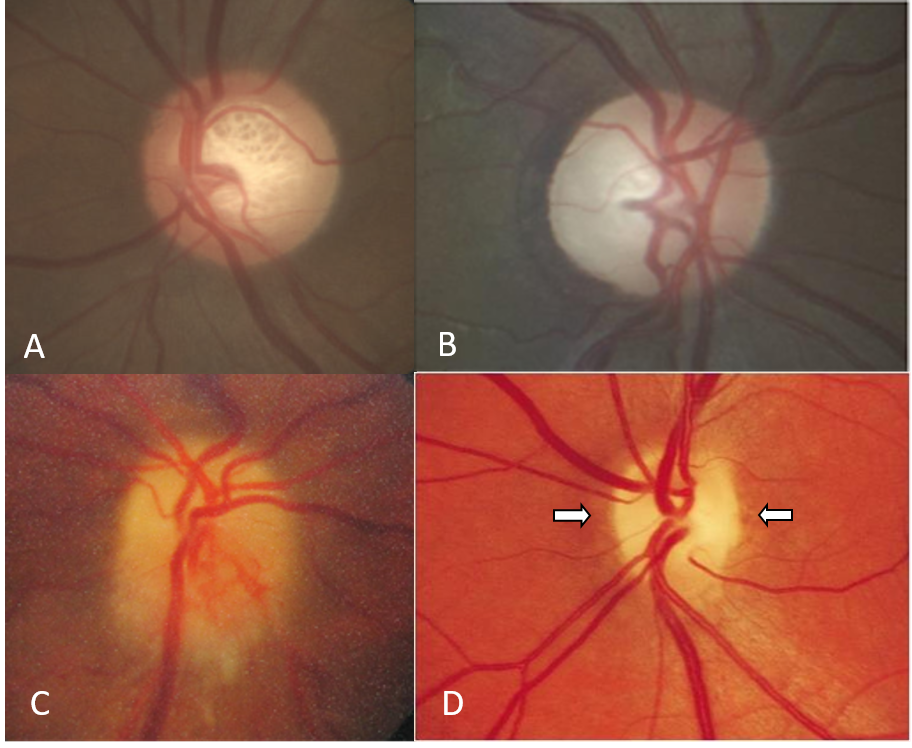
Figure 2 A.Glaucomatous disc changes B. Temporal pallor C. Sectoral pallor D. Bow tie optic atrophy
Clinical approach
It is quite common for ophthalmologists to recognize pale optic disc on routine fundus examination as an isolated entity or in association with other ocular signs with or without systemic diseases. Most commonly at the end of a detailed history and examination, we can pin the cause for optic atrophy. If it remains unexplained cause, it is better to periodically follow up such cases, just to understand the nature of vision recovery. Sometimes we can predict the cause on such follow-up. Detailed history taking is the key to decode the underlying etiology apart from comprehensive ophthalmic examination and stepwise ancillary testing.
Detailed History
History taking is of paramount importance which will guide in tailoring the investigations. The age and gender of the patient can narrow down to a list of possible causes but should be interpreted with caution. History taking is the key in identifying the probable cause of the optic neuropathy which has resulted in the disc pallor
Age
In children, the etiologies of optic atrophy may overlap with those of adults, but there could be add on causes like birth hypoxia, hydrocephalus, and other hereditary optic neuropathies.
|
Children 1 |
Adults |
Elderly |
|
Perinatal hypoxic-ischemic brain injury |
Inflammatory /infective optic neuropathies |
Ischemic /vascular causes |
|
Hydrocephalus |
Traumatic |
Compressive/infiltrative optic neuropathies |
|
Nutritional and toxic |
Intracranial or intraocular tumor |
Para neoplastic autoimmune optic neuropathy |
|
Craniosynostosis, craniofacial syndromes |
Ischemic /autoimmune optic neuropathy |
Drug-induced |
|
Non-neoplastic infiltration (neurosarcoid) |
Intracranial hypertension |
|
|
Neoplasms(tumors of the optic nerve and intracranial tumors) |
Toxic or nutritional |
|
|
Trauma |
Hereditary retinal dystrophy /Retinal vascular disease and optic atrophy |
|
|
Genetic syndromes and neurodegenerative disorders |
Hereditary optic neuropathies Neurodegenerative disorder |
|
|
Hereditary optic neuropathy |
||
|
Retinal disease and optic atrophy |
Table 5. Causes of disc pallor based on the age group.
Gender
Female preponderance is seen in demyelinating optic neuritis and certain conditions like meningioma, idiopathic intracranial hypertension, autoimmune optic neuropathies, and collagen vascular disease.
Men are commonly affected by Leber’s hereditary optic neuropathy, trauma, and toxic causes like methanol poisoning.
Ocular complaints
Acute –subacute painful vision loss, mostly pain on ocular movements, with dense central fields depression, with or without prior viral prodrome attributes a demyelinating /inflammatory etiology.
Acute painless onset vision loss is due to ischemic or traumatic and uncommonly inflammatory/infectious, etiology. A gradual, progressive vision loss is seen in compressive, nutritional, and toxic etiology
Laterality- Typical optic neuritis is usually unilateral but atypical neuritis can occur bilaterally also. Ischemic and traumatic optic neuropathy commonly unilateral. Hereditary, toxic, and nutritional optic neuropathy occurs bilaterally. Bilateral involvement indicates underlying systemic etiology.
Pediatric history taking
A thorough history of antenatal, perinatal, and postnatal events including maternal infections, maternal diabetes, prematurity, Apgar score, and history of delayed cry, neonatal seizures, and use of antiepileptic drugs is essential. History of developmental milestone should be elaborated as loss of milestones suggest degenerative and ischemic disorders. While in cases of global delay of milestones need to consider hypoxic-ischemic encephalopathy .4
Associated symptoms
History of headache, vomiting, double vision, tinnitus, and seizures suggest elevated intracranial pressure with or without compressive intracranial mass lesions. Fever, malaise, jaw claudication points to associated giant cell arteritis. History of transient ischemic attacks can be due to vascular events. Any associated motor or sensory weakness, ataxia, speech difficulty, deafness, musculoskeletal deformities should also be elicited.
Family and social history Similar vision loss in siblings or other family members favors possible hereditary cause. Smoking, alcohol or drug abuse, and sudden change in dietary habits should be noted as it can reveal a toxic or nutritional etiology.
Past medical and surgical history is important as many neuro-ophthalmic diseases are related to underlying systemic illness. Hypertension, diabetes, cardiovascular diseases, dyslipidemia, infections like tuberculosis/HIV, autoimmune diseases, malignancy and its treatment, including chemotherapy or radiation, use of antitubercular treatment like ethambutol are highly relevant and should be elaborated. Finally, a history of exposure to toxic substances like toluene in tanning factories or any other chemical exposure also should be elicited, Previous surgeries with excessive blood loss or of long duration anesthesia also can result in optic atrophy due to vascular insults.
Clinical examination
Visual acuity
The degree of vision loss may vary from mild visual impairment to no perception of light. A certain degree of nerve fiber damage can occur without obvious clinical visual loss5 and thus we may see asymptomatic patients with good visual acuity and still have optic disc pallor. Sometimes, patients may be unaware of monocular vision loss and have a pale disc, they may present when they develop fellow eye visual impairment.
Pupillary evaluation
Pupillary abnormalities are a hallmark of optic pathway dysfunction, but we have to remember retrochiasmal lesions are pupil sparing. The pupillary reaction can be sluggish or ill sustained in case of optic pathway dysfunction. The relative afferent pupillary defect is usually seen in unilateral or bilateral disease with asymmetric involvement. It can be quantified with the help of neural density filters. Both light and near reflex to be assessed in dark and light.
Color vision
Dyschromatopsia is classically seen in optic nerve dysfunction red desaturation is more common. Ishihara chart is a simple quantitative test for color vision testing. HardyRand Rittler chart is designed to test tritan defects. Red-green defects are commonly associated with disease affecting the optic nerve.
Extraocular movements may be limited in case of associated cranial nerve palsy and restriction of movements can be seen in compressive lesions.
Slit-lamp examination of the anterior segment can help to look for previous ocular trauma signs like angle recession, sphincter tear. Lisch nodules- well defined nodular iris elevations are characteristically seen in Neurofibromatosis 1. The presence of active or old inflammation like keratic precipitates or vitreous cells points towards inflammatory or infectious etiology
Fundus evaluation
Ophthalmoscopic examination of optic nerve head appearance includes the appearance of optic disc color, size, shape, cup disc ratio, neuroretinal rim peripapillary nerve fiber layer, and surrounding retinal vessels. Optic disc hypoplasia, deep physiological cup, and axial myopia can give a misleading appearance of disc pallor. Kestenbaum's capillary number sign states that the number of capillaries on the disc is less than 6 in the case of optic atrophy.
The ophthalmoscopic appearance of the disc in different types of optic atrophy is elaborated in Table 3. Though the appearance of the optic disc alone is less helpful in diagnosing the etiology, certain exceptions exist. Band or bow tie optic atrophy occurs due to chiasmal compression of crossing nasal fibers and its recognition is useful in localizing the lesion.
Diffuse or temporal pallor is often nonspecific though commonly seen in nutritional, toxic, and hereditary optic neuropathies. Associated cupping is present in methanol toxicity. Sectoral pallor is typically seen following an acute optic disc swelling in patients with non -arteritic ischemic optic neuropathy. Optic nerve sheath meningiomas and chronic papilledema may show collaterals/Opto- ciliary shunt vessels over the disc.
Focal notching, preservation of disc color, retinal nerve fiber layer defects, and cupping of disc strongly favors glaucomatous optic neuropathy
Surrounding retinal examination is mandatory to look for findings like arteriolar attenuation or sheathing, bony spicules, retinal pigment epithelial mottling, choroiditis patches or extensive PRP marks.
Systemic examination
A wide variety of systemic diseases are associated with Neuro ophthalmic conditions and hence physical examination is an essential part of work up in these patients. Frontal bossing, prognathism and enlarged, thickened hands are characteristic of acromegaly which is associated with pituitary adenoma. Poor built and cachexia indicates possible chronic illness, malignancy, or nutritional deficiency. Careful observation of facial features and dysmorphism is required as metabolic diseases like Mucopolysaccharidoses and Lipoidosis that can manifest with optic atrophy4 Skull deformity and facial asymmetry can be seen in Craniosynostosis and cranial osseous disorders (fibrous dysplasia and osteopetrosis ) They can cause optic canal stenosis and result in optic atrophy
The pallor of the bulbar conjunctiva, koilonychia, sore tongue, angular stomatitis suggest iron and vitamin deficiencies. Enlarged lymph nodes indicate underlying infection or malignancy.
Evaluation of pulse, blood pressure, heart rate, and auscultation of carotids are important in case of possible vascular or ischemic causes.
Examination of the respiratory, cardiovascular, and gastrointestinal systems has to be done to look for evidence of tuberculosis, sarcoidosis, cardiac or ischemic causes, and malignancy in appropriate cases. Basic examination of the central nervous system is an integral part of Neuro-ophthalmic evaluation and is helpful to look for associated conditions like demyelinating, inflammatory, vascular disorders, neurodegenerative diseases, and space-occupying lesions.
Skin lesions such as Café –au- lait spots, axillary freckling, and neurofibromas should raise the suspicion of neurofibromatosis.
Ocular investigation
Visual fields
Confrontation test is a rapid and simple bedside method to assess visual field loss like hemifield or altitudinal defect and central scotomas. Amsler test can be used to detect scotomas in the central 20 degrees. Goldman perimetry is the ideal perimetry for neuro-ophthalmic examination but it is mostly replaced by the newer generation Perimeters like Humphreys analyzer. Humphrey visual field 30-2 program is used commonly to detect visual field defects. The specific pattern of visual field defect is helpful in the differential diagnosis. Toxic, nutritional, and hereditary optic neuropathy produces central or ceco-central scotomas (commonly bilateral and symmetrical). In optic neuritis, generalized constriction, three quadrant defects, central scotomas, or altitudinal defects are seen. Ischemic optic neuropathy typically produces altitudinal defects either superior or inferior. Chiasmal lesions characteristically show bitemporal hemianopia. Posterior visual pathway and occipital lesions produce homonymous defects.
Contrast sensitivity
Loss of contrast sensitivity is seen in diseases affecting the optic nerve and is measured by the Pelli-Robson chart and Vistech chart.
Optical Coherence Tomography
It shows structural changes in the optic nerve and retinal layers. Retinal nerve fiber layer thinning and ganglion cell loss happens in optic atrophy and useful for documentation and follow-up. Ganglion cell layer loss happens earlier than RNFL loss in optic atrophy
Visual Evoked Potential gives information regarding the integrity of the visual pathway. Delayed P1 latency is seen in optic neuritis and useful to assess subclinical involvement of the fellow eye. In compressive optic neuropathy, there is prolonged latency in the early-stage, although not to the extent seen in optic neuritis. In ischemic optic neuropathy, the amplitude is reduced but latency is not significantly delayed.
Electroretinogram is helpful in case of associated retinal dysfunction as in the case of heredomacular degeneration, macular toxicity, vascular occlusion, etc. Extinguished waveforms are seen in retinitis pigmentosa. In the pattern, ERG P50 reflects the macular photoreceptor function and N95 is related to retinal ganglion cell function. The N95:P50 ratio is decreased in optic nerve diseases while the ratio is normal in maculopathy.6 ERG is useful in cancer-associated retinopathy, retinitis pigmentosa, cone dystrophy, and toxic retinopathies.
Neuroimaging
A multicentric study 7 by AG Lee et al evaluated 91 patients with isolated, unexplained optic atrophy and identified compressive lesions in 18 (20%). Hence they recommend neuroimaging in all patients with unexplained optic atrophy. MRI brain and orbit is the imaging modality of choice for the optic nerve and intracranial visual pathway lesions. Neuroimaging plays a vital role in optic neuritis evaluation to detect brain demyelinating lesions. Adequate sections with fluid-attenuated inversion recovery (FLAIR ) sequences and post-contrast fat-suppressed images are needed to look for optic nerve signals. Optic nerve tumors and intracranial mass lesions are best visualized on post-contrast MRI brain and orbit cuts. MRA and MRV Brain are indicated to assess vascular malformations and cerebral venous sinus abnormalities respectively.CT Brain and orbit has a role in case of trauma, skeletal abnormalities (microcephaly, osteoporosis), and in conditions when MRI is contraindicated or claustrophobic patients.
Systemic investigations
A detailed history and clinical examination can narrow down the diagnostic possibilities and systemic investigations. Complete hemogram, blood sugar, lipid profile, S.Homocysteine, and procoagulant risk factors, C reactive protein, temporal artery biopsy (for arteritic AION), and Carotid Doppler and MRA neck can be used for screening carotid artery diseases in case of ischemic or vascular etiology. In the case of atypical neuritis associated optic atrophy, laboratory tests include Mantoux, chest X-ray, sarcoid workup, VDRL, TPHA, Elisa for HIV, and autoimmune workup. Aquaporin 4 antibody and MOG antibody test and MRI spine have to be included for Neuromyelitis Optica and recurrent neuritis.
In thyroid eye disease, free T3, T4, TSH, and TPO antibodies are measured. In the case of nutritional optic neuropathy, assessment of Serum Vitamin B12, RBC-folate and S.Hemoglobin may prove useful. Paraneoplastic panel of antibodies is recommended for paraneoplastic optic neuropathy. Whole-body screening including mammogram, PAP smear, and as well as a whole-body PET may be needed in case of an infiltrative etiology. Genetic counseling and testing for mutational analysis either specific or whole-genome sequencing is required in cases of hereditary optic atrophy (Leber’s hereditary optic atrophy, Dominant optic atrophy), Wolfram syndrome, and hereditary retinal disease).
Case Example 1
A 53 –year old male presented with gradual painless vision drop both eyes since 3-4 years. On Fundus examination, both optic discs were pale. Visual field testing showed bitemporal hemianopia and OCT documented thinning of RNFL and GCC layer. MRI revealed pituitary macroadenoma causing compressive optic neuropathy. Fig 3 &4
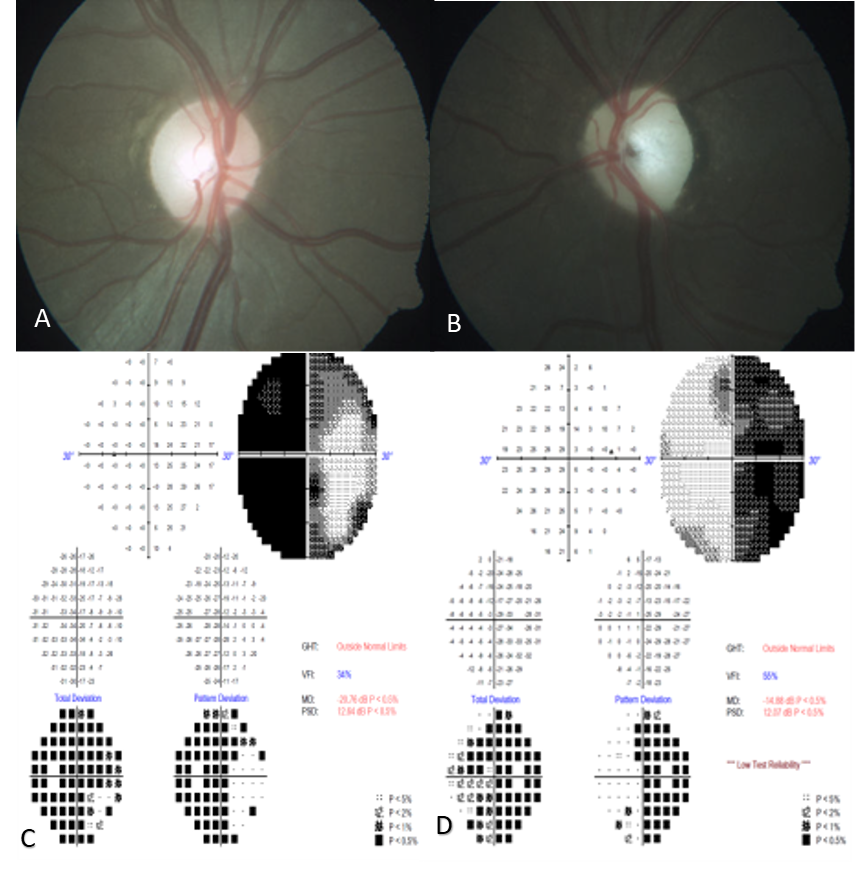
Figure 3 A& B. Fundus photograph of both eyes. C & D. Humphrey visual fields – Bitemporal hemianopia
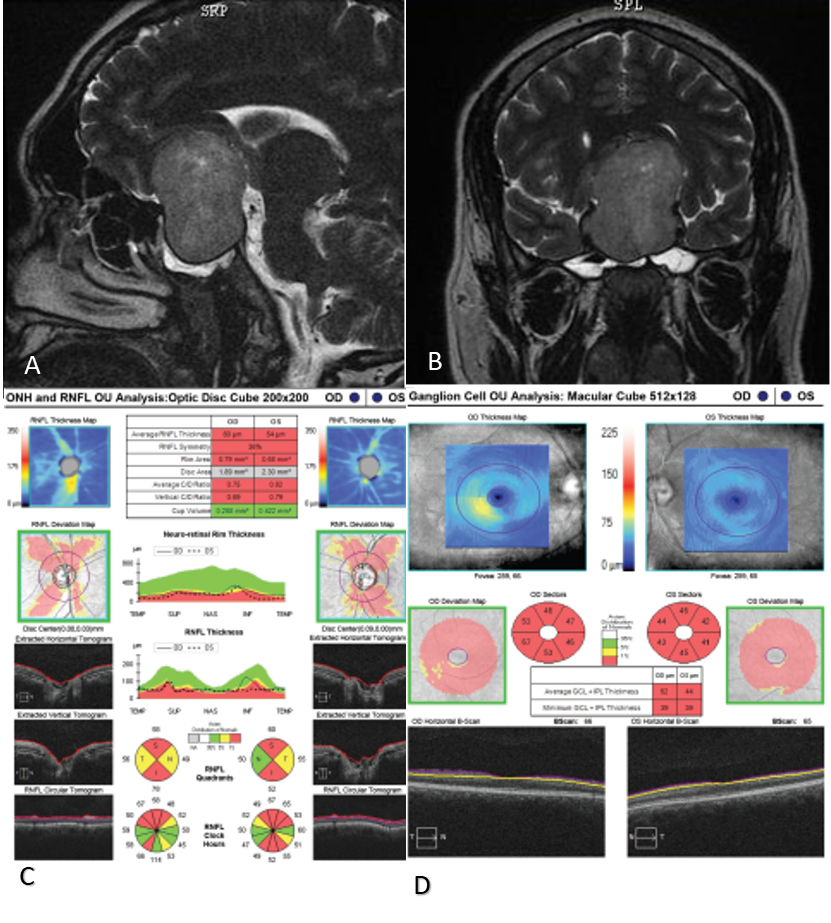
Figure 4 A&B: MRI Brain- Saggital and coronal cuts showing huge sellar suprasellar pituitary adenoma, C & D: OCT optic nerve and macula –gross thining of RN FL, GCC
Case Example 2
A 32-year-old male came with complaints of bilateral vision loss following consumption of contaminated alcohol. His visual acuity was 6/60 in the right eye and left eye 2/60 with pale and cupped optic discs. MRI revealed putaminal necrosis FIG 5
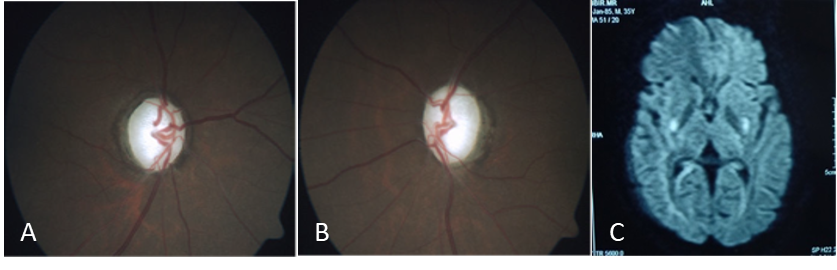
Figure 5 A & B Toxic optic atrophy C. MRI DWI sequence –showing putamen necrosis
Case Example 3
A 15-year-old female presented with the gradual diminution of vision for 2 years. Her visual acuity was 2/60 in both eyes and her younger brother also had a similar vision problem. Fundus showed bilateral temporal disc pallor with RPE alterations at macular and retinal flecks probably due to heridomacular degeneration which was confirmed on autofluorescence (Stargardt’s disease) Figure 6
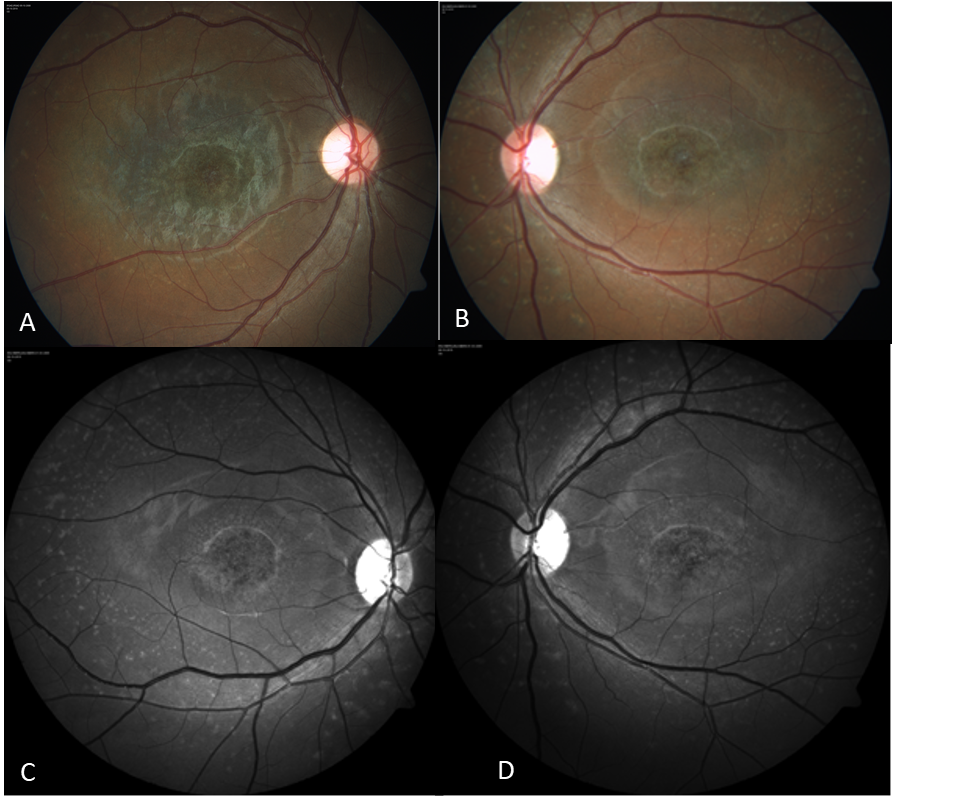
Figure 6 A & B. Fundus photograph showing temporal pallor with retinal flecks C & D Autofluorescence –Red free images
Case Example 4
A young male with a history of road traffic accident 6 months presented with diminution of vision in the left eye. On examination, there was left optic disc pallor and CT orbit revealed left optic canal fracture.(Fig 7)
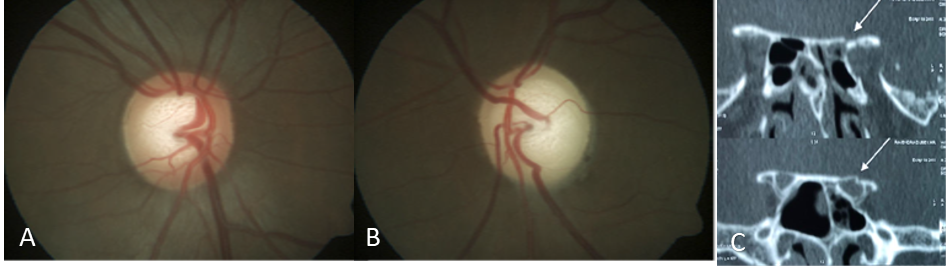
Figure 7 A& B. Photograph showing normal disc in right eye and optic disc pallor in the left eye C. Coronal CT Bone window – showing optic canal fracture
Case Example 5
A 45 year old female came with complaints of left eye gradual diminution of vision -10 months. Visual acuity was 6/6 in right eye and CFCF in left eye. OD had the normal optic disc , OS showed pale disc with opto ciliary shunt . MRI brain and orbit revealed thickened and enhancing left optic nerve sheath suggestive of Optic nerve sheath meningioma along with right frontal convexity meningioma FIG 8
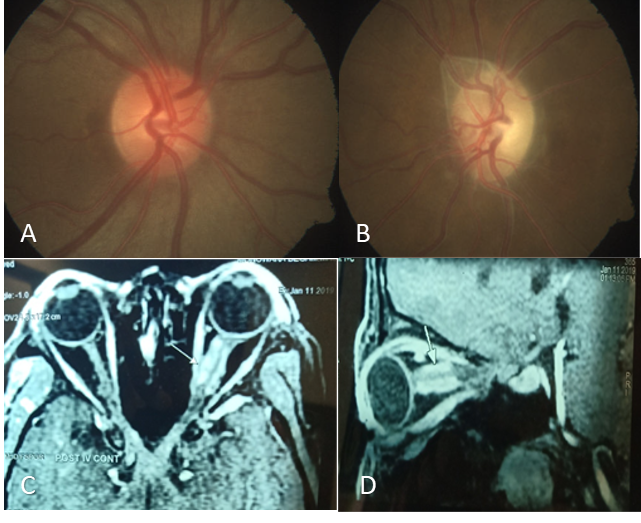
Figure 8: A & B: Photographs showing normal disc in the right eye and pale disc with optociliary shunt C & D: Axial and sagittal MRI Orbit suggestive of classical tram track sign optic nerve sheath meningioma
Case Example 6
A 46-year-old male presented with painless progressive vision drop in both eyes since 20days.His visual acuity was NPL in the right eye and PL in the left eye with bilateral optic disc pallor. MRI brain and orbit with MRA revealed a large saccular partially thrombotic aneurysm arising from right supraclinoid ICA. (Figure 9)
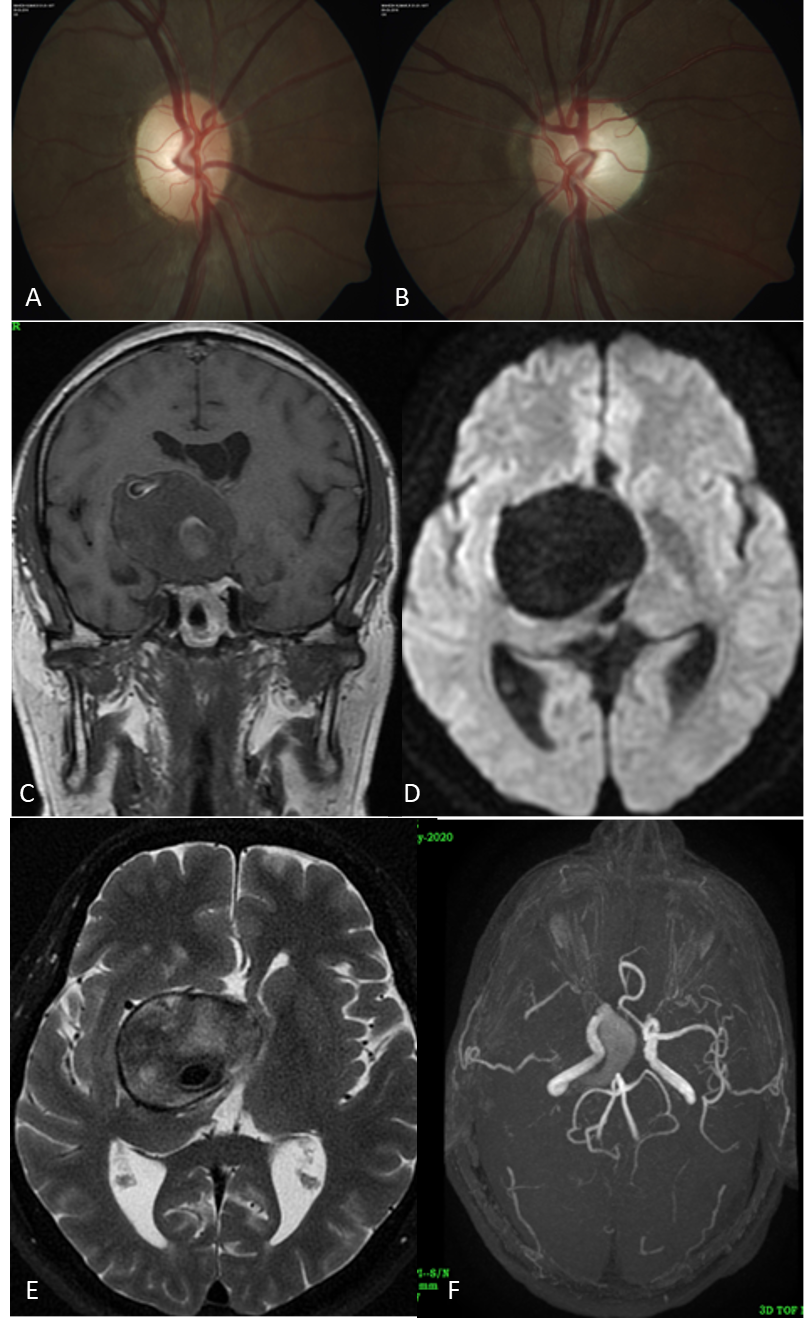
Figure 9: A & B: Fundus photograph showing pale disc in both eyes C & D. MRI Brain, E & F: MRA suggestive of huge right surpaclinoid ICA aneurysm
Conclusion
Optic disc pallor is commonly seen in clinical practice and its evaluation poses challenges to ophthalmologists. Patients can present with mild visual impairment to total blindness with disc pallor. Disc pallor can be seen incidentally during a routine examination. A systematic approach including a thorough history and comprehensive ocular examination along with tailored investigations will help ophthalmologists to pin the diagnosis of optic atrophy in most cases. Though effective treatment is limited inmajority of patients and the visual prognosis is guarded in view of the irreversible nature, it is important to prevent similar damage to the fellow eye. Occupational rehabilitation, low visual aids may be fruitful and appropriate for a few cases. Neuroprotective agents, stem cell therapy, and artificial devices are the key for future treatment options for these shades of white !!.
Acknowledgments
I sincerely acknowledge Dr. Padmalakshmi Krishna Kumar who helped in collecting images and content for this article.
References
1.McClard CK, Shah V. Pediatric Optic Disc Pallor. IntOphthalmolClin. 2018 Fall;58(4):125-145. 2.Rose FC.Optic Atrophy.Postgraduate Medical Journal.1964Dec 1;40(470):692-5. 3.Dastoor H D. Srinivasan oration- a study of optic atrophy. Indian J Ophthalmol 1966;14:55-74 4. Liu GT, Volpe NJ, Galetta SL. Neuro-ophthalmology Diagnosis and Management. 2nd edition. 5.Ouvrier RA. Pallor of the optic disc in children. Aust N Z J Ophthalmol. 1990 Nov;18(4):375-9. 6.Sen P, Sachidanandam R. Recent Advancements in Ocular Electrodiagnostics. Medical & Vision research foundations. 2015 Jun;33(2):83. 7.Lee AG, Chau FY, Golnik KC, Cardon RH, Wall M. The diagnostic yield of the evaluation for isolated unexplained optic atrophy. Ophthalmology 2005:112:757-59.