.jpg)


1. History
A careful history helps in identifying the etiology of ptosis (Fig 1). The age at onset of ptosis and its duration will usually distinguish congenital from acquired cases. Relevant history should be elicited in all patients regarding the variability of ptosis during the day, associations with any jaw movements, abnormal ocular movements and head posture, diplopia, or tiredness. Old photographs often reveal important information. A family history of similar conditions should be determined to rule out Congenital or hereditary ptosis, blepharophimosis, ocular myopathies, etc. Any history of previous surgery, trauma, or use of steroids should be recorded. According to its etiology, it can be classified as myogenic, aponeurotic, neurogenic, neuromuscular, mechanical, or traumatic.
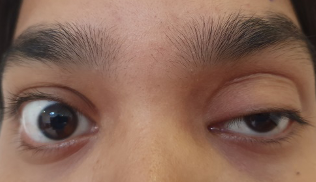
Figure 1: Young female with Left eye severe ptosis
2. Ruling out pseudoptosis
There are conditions that can mimic ptosis include enophthalmos, anophthalmos, contralateral proptosis, contralateral lid retraction, dermatochalasis, hypotropia, facial nerve palsy, superior sulcus deformity, and brow ptosis. The proper examination helps to differentiate these conditions from that of true ptosis.
3. Observation
Examination starts from the moment a patient enters the doctor’s chamber. Head posture and face turn, if any, should be noted. The chin-up position is the most commonly encountered posture. The presence of frontalis overaction should be noted, as the patient may compensate for the ptosis by lifting eyebrows with the frontalis muscle.
3. Measurements
Measuring these parameters mentioned below, not only helps in grading the ptosis but also helps in deciding the type of surgery required.
A. Palpebral aperture:The measurement of the palpebral aperture ( both horizontal & vertical ) is necessary as the difference between the two eyes gives the measurement of the ptosis in unilateral cases or the difference from the normal in the bilateral cases (fig 2). Normal measurement is 9-10 mm in primary gaze. However, judging the amount of ptosis by the difference in the size of the palpebral aperture has limitations due to possible alterations in the position of the lower eyelid.

Figure 2: Measurement of the vertical palpebralaperture
B. Margin–reflex distance1 (MRD1) The distance between the upper eyelid margin and the corneal reflex of a pen torchlight held by the examiner on which the patient fixates; the normal measurement is 4–5 mm (fig 3 a & b). The difference in MRD 1 of the two sides in unilateral cases or the difference from normal in bilateral cases gives the amount of ptosis.
The amount of ptosis may be classified as Mild ptosis – 2mm or less, Moderate ptosis – 3mm and Severe ptosis, if 4mm or more.
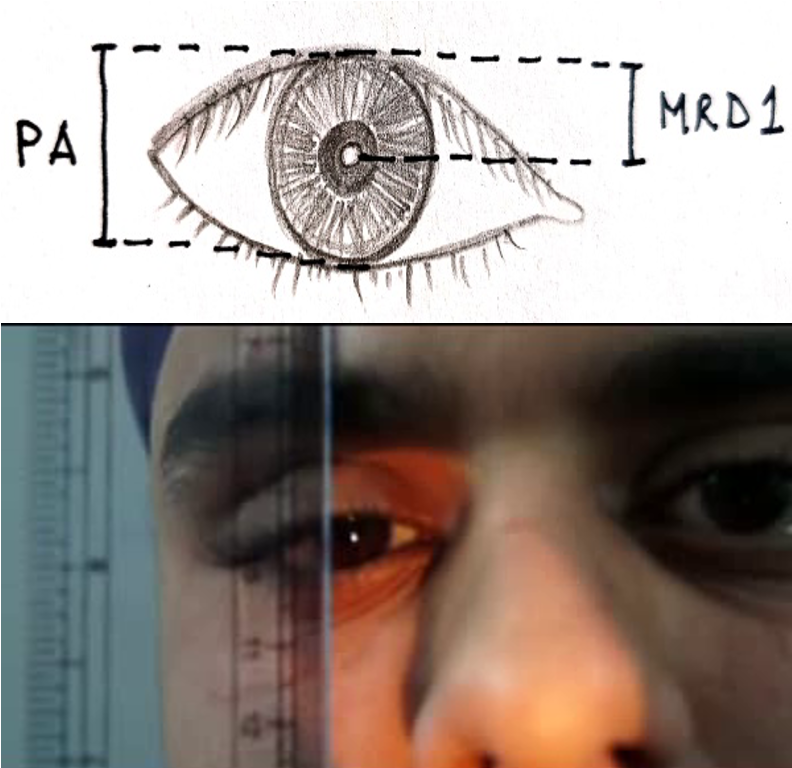
Figure 3 Measurement of MRD1, distance from corneal light reflex to the upper eyelid margin
C. MRD2 – The distance from lower eyelid margin to corneal light reflex in primary gaze. Aids in comparing true eyelid position. Normal: 4.0–5.0 mm.
D. Levator function (upper lid excursion)is measured by placing a thumb firmly against the patient’s brow to negate the action of the frontalis muscle. The patient is then asked to look down first and then extreme up. The amount of excursion is measured with a rule (fig 4 ).
Levator function may be graded as excellent (>10 mm), good (9 mm or 10 mm), fair (5–8 mm), and poor (4 mm or less).
Diagram showing the levator function measurement by noting the excurcision of the eyelid from downgaze to extreme upgaze after blocking the action of the frontalis muscle.
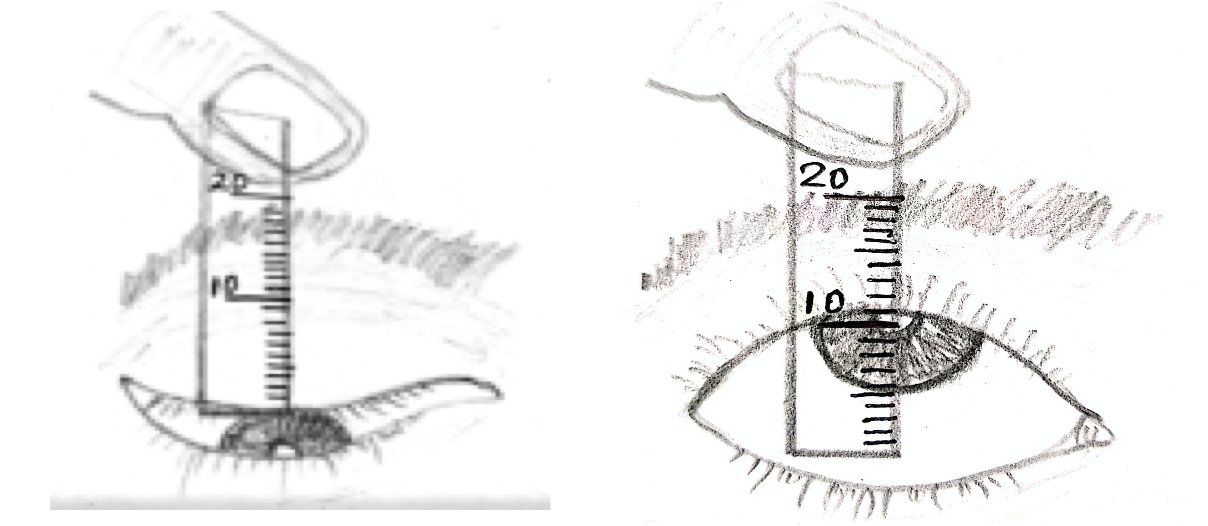
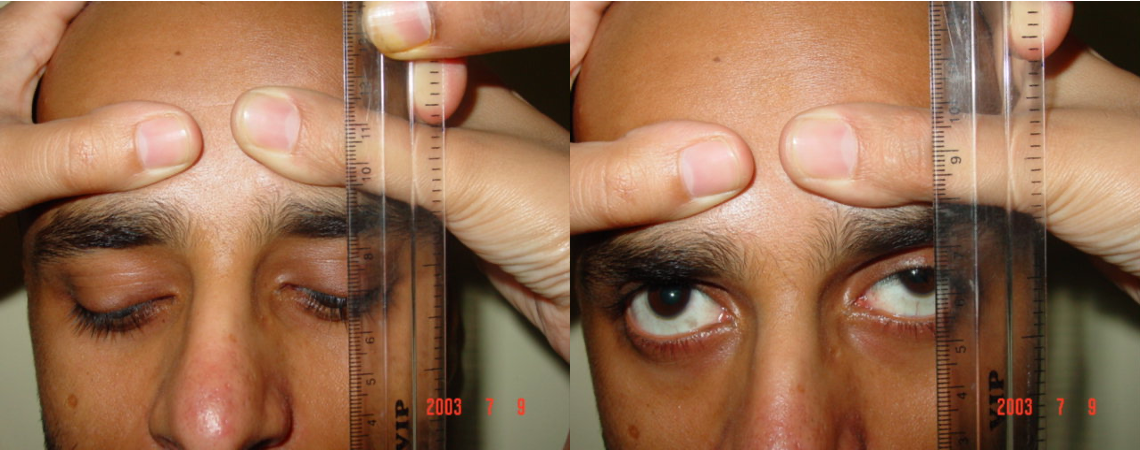
Figure 4 Measurement of levator function
E. Margin Crease Distance (MCD)Measurement of the margin crease distance (MCD) is the next important step in the examination. The height of the eyelid crease in downgaze should be measured on the ptotic side and compared to the normal eyelid in downgaze ( Fig 5). MCD in normal eyes is 5-7 mm. The distance of the lid crease from the margin is measured as it helps in planning the surgical incision. Also, presence of a distant lid fold in a case of moderate to severe ptosis with good levator action indicates a levator aponeurotic dehiscence.

Figure 5 Measurement of margin crease distance in downgaze
F. Tarsal platform show (TPS)is an important measurement as it is of great aesthetic significance. It is the apparent distance of the crease from the center of the eyelid margin in the primary position.
G. Bell’s phenomenonis the upward rotation of eyeball on the closure of the eye ( Fig 6). Confirmation of the presence of Bell’s phenomenon is important before undertaking any surgical procedure to avoid the risk of postoperative exposure keratopathy.
Figure Assessment of Bell’s Phenomenon
4. Associated signs
- Best-corrected visual acuity should be checked to record the presence of amblyopia in the ptotic eye.
- Pupils should be examined to exclude Horner syndrome and pupil-involving third nerve palsy.
- Lagophthalmos should be noted. The presence of lagophthalmos is an indication of potential corneal exposure following ptosis repair.
- Ocular motility defects, particularly of the superior rectus or mono-ocular elevation defect, must be evaluated in patients with congenital ptosis. Correction of an ipsilateral hypotropia may improve the degree of ptosis.
- Jaw-winking should be identified by asking the patient to open the mouth or chew and move the jaws from side to side ( FIG 7 a & b).
- Measurement of the horizontal length of the palpebral fissure, intermedial canthal distance (ICD), and interpupillary distance (IPD) helps in the diagnosis of telecanthus (ICD < ½ of IPD) associated with blepharophimosis syndrome ( Fig 8).

Figure 7 Four-year-old child with severe jaw winking ptosis, elicited on the wide opening of the mouth

Figure 8: A young child with Blepharophimosis syndrome
6. Assessment in Children
Measurement of levator function in small children is a difficult task as no formal evaluation is allowed by the child. The presence of lid fold and increase or decrease in its size on the movement of the eyelid gives us a clue to the levator action. The presence of anomalous head posture like the child throwing his head back suggests a poor levator action.
Iliff Test - This is another indicator of levator action. It is applicable in first year of life. The upper eyelid of the child is everted as the child looks down. If the levator action is good, the eyelid reverts back on its own.
7. Don't forget these Tests
- Phenylephrine test: Sympathomimetic agents, such as phenylephrine 2.5% (or 5%) drops are used to assess mild cases of ptosis as in Horner's syndrome. The positive phenylephrine test suggests that the patient would respond well to Muller's muscle resection.
- Schirmer’s test ( Fig 9) and Tear breakup time should be performed in individuals suspected of having dry eyes due to the potential risk of incomplete eyelid closure and exposure keratopathy following surgical correction.
- Corneal sensitivity - The presence or absence of corneal functions should be noted using a cotton wisp ( Fig 10).

Figure 9 Schirmer’s test to rule out dry eyes

Figure 10 Assessment of Corneal sensation
8. Ruling out Myasthenia gravis
Fatigue test: Fatigability is tested by asking the patient to look up without blinking for 30–60 seconds. Progressive drooping of one or both lids, or an inability to maintain upgaze, is suggestive of myasthenia gravis.
Cogan’s lid twitch: Elicited by having the patient look in downgaze, followed by upgaze. As the affected eye saccades up, the upper lid overshoots. Seen in myasthenia.
Ice test: Glove containing ice pack is applied on the closed ptotic eye for 2 min. If the lid elevates by 2 mm or more, it is suggestive of myasthenia ( Figure 11).

Figure 11: Ice test to rule out Myasthenia Gravis
Tensilon test: This test is done in doubtful cases of suspected myasthenia, 2 mg of edrophonium is injected slowly in 15–30 s. The needle is left in situ, and the remaining 8 mg is injected slowly if no adverse reaction is observed within 1 min. If myasthenia is the cause, ptosis improves after the injection. However, because of difficulty in availability of edrophonium, Neostigmine test is often used. In adults, 1 mg of neostigmine is injected I/M. The ptosis improves in 5 to 15 minutes if Myasthenia gravis is the cause.
9. Herring’s law
Herring’s law of equal innervation states that the reciprocal eye muscle of each eye is innervated equally. Hence, the manual elevation of the more ptotic eyelid decreases the muscle strength required to keep the lid elevated, and so the contralateral LPS relaxes and causes ptosis in the other eye. If this occurs, the patient should be warned that surgical correction may induce a lower position in the opposite lid.
10. Management based on evaluation
Our surgical approach depends on the evaluation of its etiology, on whether it is unilateral or bilateral, the severity of Ptosis, levator action and presence or absence of abnormal ocular movements, jaw winking phenomena, or blepharophimosis syndrome. Hence, a proper and thorough evaluation is an essential aid in deciding the surgical approach.