
Introduction
Open globe injuries (OGI) are associated with retained intraocular foreign body (IOFB)in 18 to 41% of cases1. Retained IOFB is an important cause of visual morbidity and blindness, especially in working-age population with male predominance. Majority of the IOFBs are related to trauma at workplace1.
Types of IOFB
Majority of IOFB are metallic1,2. It is followed by organic IOFB and metallic non magnetic IOFB. Metallic IOFB like iron or copper can cause metallosis leading to poorer visual outcomes if left untreated. Organic IOFB are associated with high incidence of fungal endophthalmitis and need treatment on emergency basis. Inert IOFB like glass or noble metal like gold can be present in a minority of patients. Theoretically these can be managed conservatively, however with advancements in Vitreoretinal Surgery it is seldom done.
Location of IOFB
Most common resting place for IOFB is vitreous cavity. Though it may be lodged in any part of the eye. IOFB might be present in anterior chamber, intralenticular, vitreous cavity or even orbit. It's essential to determine exact location of IOFB preoperatively as it be may be difficult to detect certain IOFB intraoperatively. IOFB lodged in anterior chamber angle or in pars plana region may be missed unless thorough preoperative evaluation is done.
Preoperative evaluation
History
Detailed history of the patient is essential part of preoperative evaluation and must be elicited prior to clinical examination. History taking should involve circumstances of injury, place of injury ( whether related to workplace), use of protective eyeware or prescription glasses ( latter may lead to glass IOFB), history of assault, time of injury ( important to document time elapsed between occurrence of injury and presentation at clinic), any prior intervention or medication used.
It's important to determine the type of IOFB if possible. It helps to determine the possibility of complications like endophthalmitis associated with vegetative IOFB.Thorough ocular and systemic history must be ensured. Any history of prior ocular disease or ophthalmic surgery helps in planning surgical approach e.g. in case of a patient with glaucoma conjunctival handling should be more careful while doing vitrectomy for posterior segment IOFB. Detailed systemic history is important to determine any comorbidities e.g. uncontrolled diabetes mellitus or hypertension.
History of associated head injury must be specifically asked for and documented. Medico-legal implications must be kept in mind and necessary documentation done. If it is necessary to inform law enforcement agencies, it should be done after primary care has been given to the patient. Preservation of documentation can't be emphasized enough, as many times a surgeon may be called to give evidence in court of law after a significant time interval and asked to produce documents.
Clinical examination
Best-corrected visual acuity of involved and uninvolved eye must be evaluated before doing any further examination. Even in bedridden patients with polytrauma, bedside visual acuity evaluation should be done.
External examination to look for orbital findings is carried out. Presence of retrobulbar hemorrhage, periorbital hematoma, lacerations of lids and adnexa, any FB in adnexal region ( in blast injuries), orbital fracture must be ruled out. Canalicular tears should be looked for and confirmed as it requires careful management.
Slit Lamp biomicroscopy should be done to ascertain anterior segment involvement. Lacerations of conjunctiva or gross chemosis, latter may be indicative of occult globe rupture, partial thickness or full thickness corneal laceration should be ascertained with siedel's test. Presence of reaction in anterior chamber, fibrin,hyphema, hypopyon or leaked lenticular material evaluated. Anterior chamber depth should be checked. It might be shallow or even flat with iridocorneal touch in presence of leaking corneal wound. It might be normal if the corneal leak is self-sealed. Pupillary reaction should be checked, and afferent pupillary defect confirmed. Peaked pupils should raise suspicion of OGI. Presence of transillumination iris defects are indicative of posterior segment IOFB.
An IOFB can lead to variable lenticular findings. Breach of anterior capsule is associated with cataract formation and leakage of lens matter in AC seen as wrinkling of anterior capsule. Zonulolysis and lens subluxation must be ruled out.
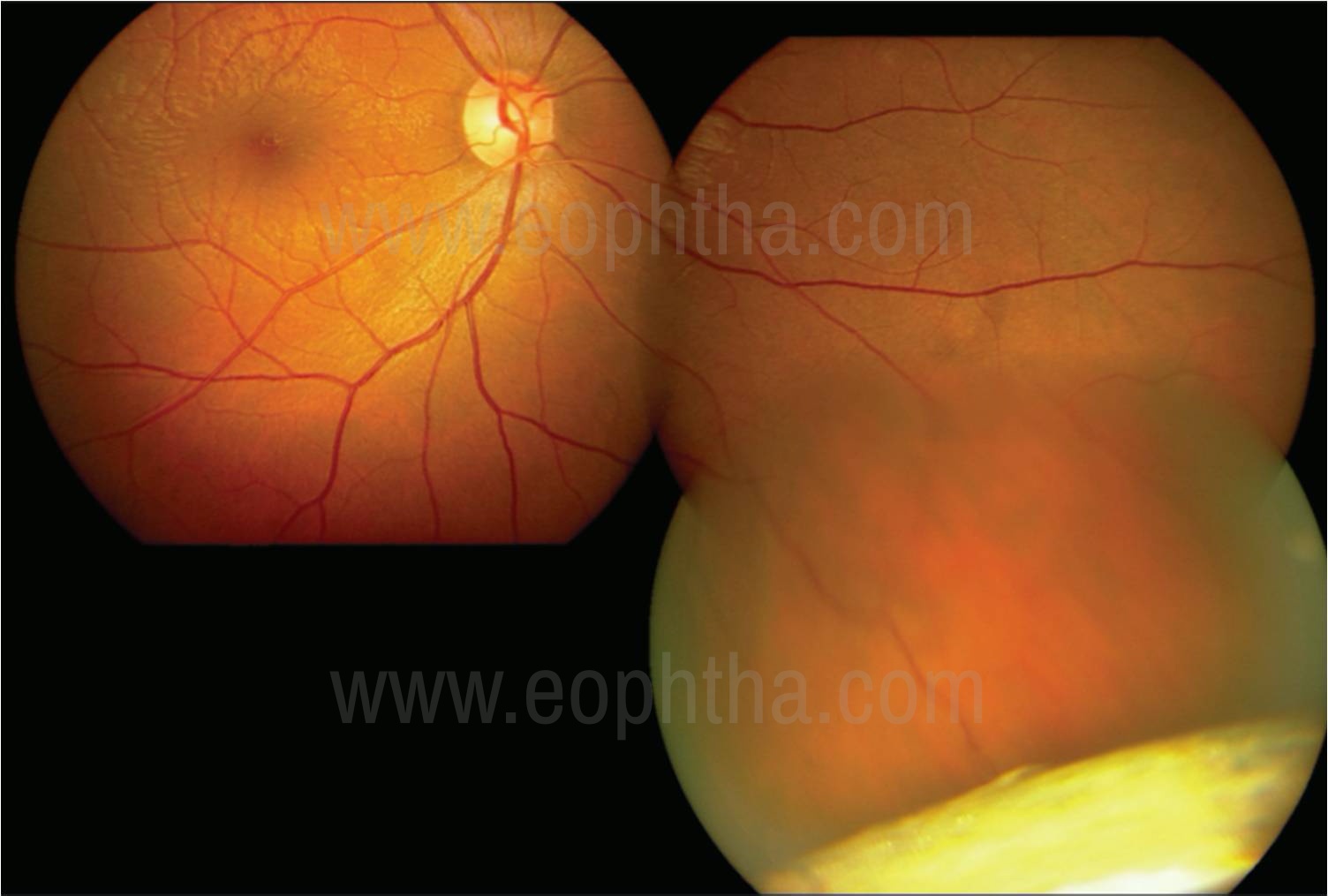
Posterior segment should be thoroughly evaluated after pupillary dilatation, if fundus view is present. Vitreous hemorrhage, commotio retinae, retinal tear, retinal dialysis or retinal detachment should be looked for. The presence of choroidal detachment or choroidal tear should be noted. If IOFB (Fig.1) is visible, its size, shape, possible material, location in the eye, choroidal impaction etc should be noted. It IOFB is present in vitreous cavity or lying on retinal surface, possibility of retinal tear formation between time of assessment and time of surgery is possible.
Imaging
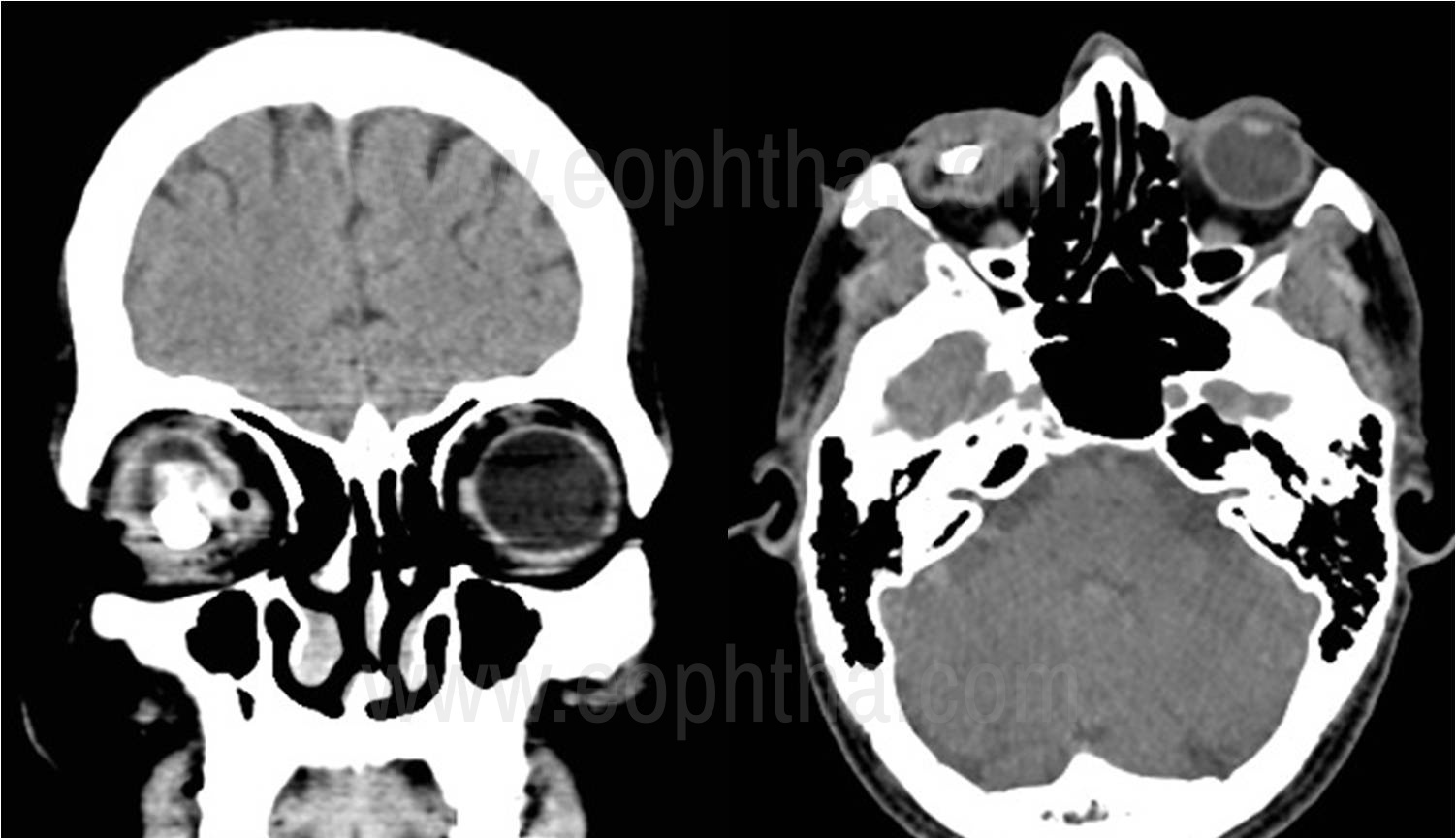
CT scan (Fig.2) is the most helpful and most commonly used imaging modality. It helps to detect a wide range of IOFBs3, with possible exception of vegetative or orbital FB. Surgeons must ask for 1mm sections of CT as standard 5 or 10mm sections have risk of missing the IOFB. Coronal, axial and sagittal views should be taken to ascertain relative position of IOFB wrt to other intraocular structures. Nature of IOFB can be judged based on appearance and measurement of Hounsfeld units. CT scan also gives important information about integrity of globe, position of lens, state of posterior capsule, presence of retinal detachment etc. Paranasal sinuses should also be imaged to rule out any orbital FB or fractures.
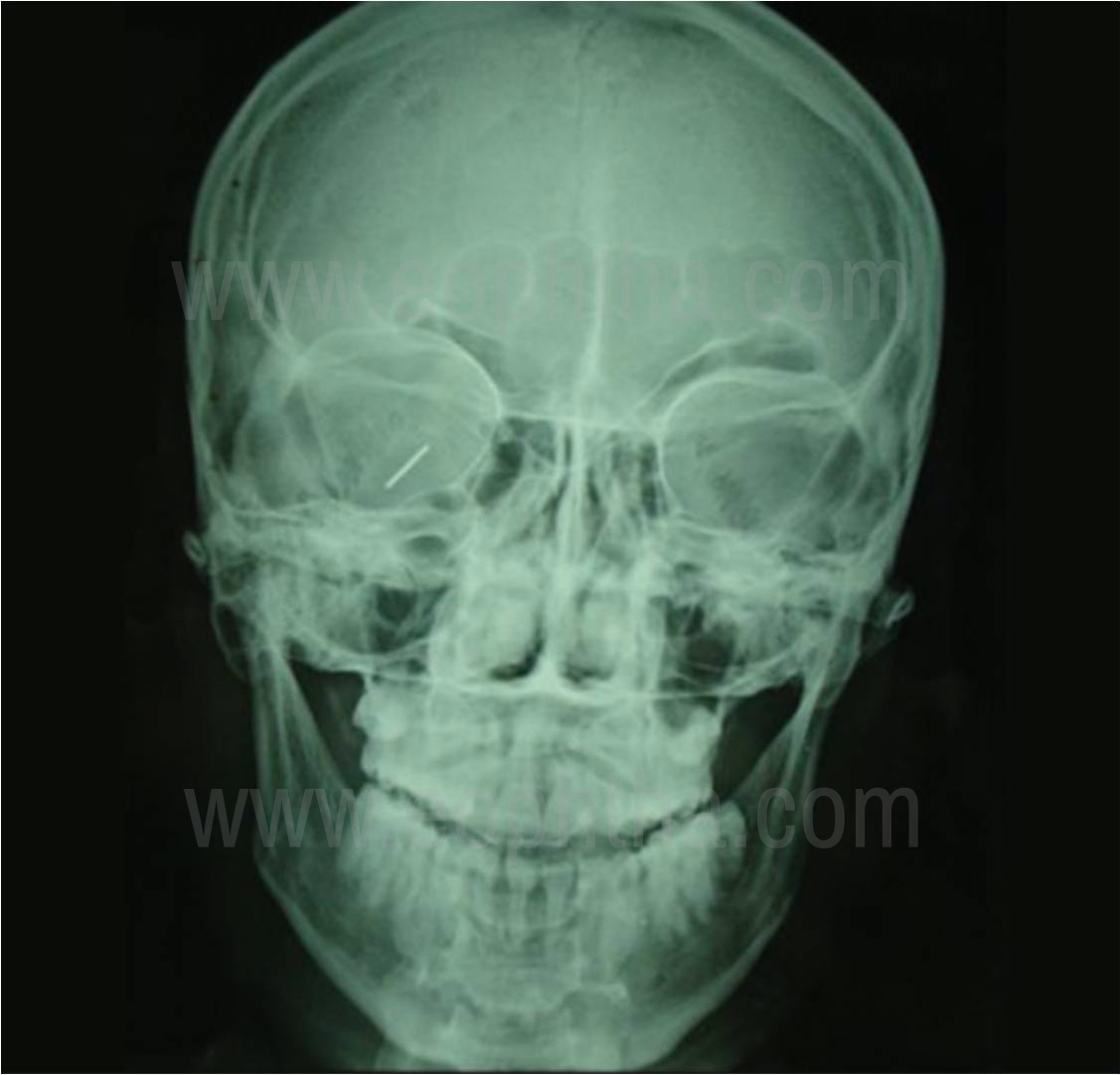
X-ray (Fig.3) is useful to ascertain presence or absence of IOFB in absence of easy access to CT scan. However it does not provide specific details regarding relative position of IOFB when compared to intraocular structures. Hence it is not of much value in planning surgical approach.
B- scan ultrasonography is commonly used imaging technique. It is generally avoided in the presence of an open globe. But it can give useful information about the posterior segment like presence or absence of posterior vitreous detachment or retinal detachment, nature and relative position of IOFB.
MRI is generally avoided in trauma cases due to the possibility of ferromagnetic IOFB.
Pre-op consideration
Topical medication is usually avoided if globe is open. Patient should be started on oral and parenteral broad-spectrum antibiotics. Status of tetanus immunization should be assessed and immunization is given if necessary. The patient should be asked to maintain nil per oral status till he can be taken to OR.
Counseling
Prior to surgery, a patient with IOFB should be counseled about the severity of trauma and nature of surgery planned. Poor visual acuity at presentation and posterior segment IOFB are poor prognostic factors4.
However, patients must be made aware of possible adverse events like retinal detachment or endophthalmitis, especially in posterior segment IOFB. Possibility of multiple surgeries, permanent visual disability, variable visual prognosis, and sympathetic ophthalmia should be clearly explained and consent should be taken for the same.
Timing of Surgery
In the case of IOFB, usually, it's removal is done as a primary procedure along with primary wound repair. In the case of associated endophthalmitis as well, it is performed as the primary procedure. However in case of posterior segment IOFB if the patient has already undergone primary wound repair elsewhere and there are no signs of infections or risk of retinal complications, surgery can be postponed for about 2 weeks. Over a period of 2 weeks, the development of PVD takes place and benefits surgical outcome.
Anesthesia
General anesthesia is preferred. However local anesthesia along with sedation can be used in select cases5. It is preferable to use parabulbar anesthesia under microscope visualization rather than peribulbar block which is a blind procedure and can greatly increase intraorbital pressure.
Surgical considerations
Assessment and closure of the entry wound have to be the first surgical step. Corneal suturing is done with 10-0 nylon sutures while for scleral wounds 6-0 or 7-0 vicryl sutures are used. The posterior extent of the scleral wound must be explored and sutured under vision before proceeding to Vitreoretinal management.
Anterior segment IOFB
IOFB that can be visualized easily can are removed using serrated straight forceps used by Vitreoretinal surgeons via paracentesis incisions. The IOFB should be directed along its long axis so that it can be removed via paracentesis, which in turn can be enlarged for ease of removal. Endothelium must be protected using viscoelastic material. Viscoelastic also helps to maintain anterior chamber depth while IOFB is being removed. Large and irregular IOFB may have to be delivered through the scleral tunnel so as to maintain watertight wound post-op.
If IOFB is small and not visualized easily, intraoperative gonioscopy lenses ( e.g. Swan- Jacob gonio lens) should be used to locate it in anterior chamber angle.
While managing intralenticular IOFB, the status of the posterior capsule is important. If the posterior capsule is breached, the surgeon should be prepared for 3 post pars plana vitrectomy (PPV) should IOFB &/or lens material drop in the vitreous cavity. However, if the posterior capsule is intact, phacoemulsification can be safely done & IOFB removed through phacoemulsification incision. The primary placement of IOL is generally deferred due to the risk of endophthalmitis. Secondary IOL placement also gives an opportunity for more accurate IOL power calculation prior to IOL placement.
Posterior segment IOFB
PPV with internal removal of IOFB is a standard method of management in these cases. Prior to posterior segment intervention, the anterior segment has to be cleared of hyphema, exudates, and lens material to get a clear view of the vitreous cavity. Complete vitrectomy is done to release the IOFB of all vitreous attachments. Any traction on the retina must be ruled out. IOFB is lifted from the retinal surface and removed from the eye. Latter 2 steps depend on the characteristics of IOFB like size, shape, magnetic or not, etc.
In the first step, complete vitrectomy is performed to free the IOFB of all attachments. If IOFB is covered with a fibrotic capsule, the capsule is cut with a cutter or vitreous scissors. For IOFB impacted in the choroid, laser burns are given around the IOFB before removal from the site of impaction due to the risk of massive choroidal hemorrhage. If IOFB is not easily visible due to hemorrhage or exudates in endophthalmitis, it is advisable to use chandelier light source and perform the examination of the retinal periphery with external depression. Generally, such IOFBs are retained in the pars plana region and have to be free of attachments with the vitrectomy cutter. Induction of PVD can be performed either prior to the removal of IOFB or after. The author prefers to induce PVD after IOFB removal as the sheet of posterior hyaloid reduces the impact of retinal trauma in case IOFB falls to the retinal surface. Liquid perfluorocarbon (LPFC) is often used to float the IOFB & to reduce impact trauma if IOFB falls on the retinal surface.

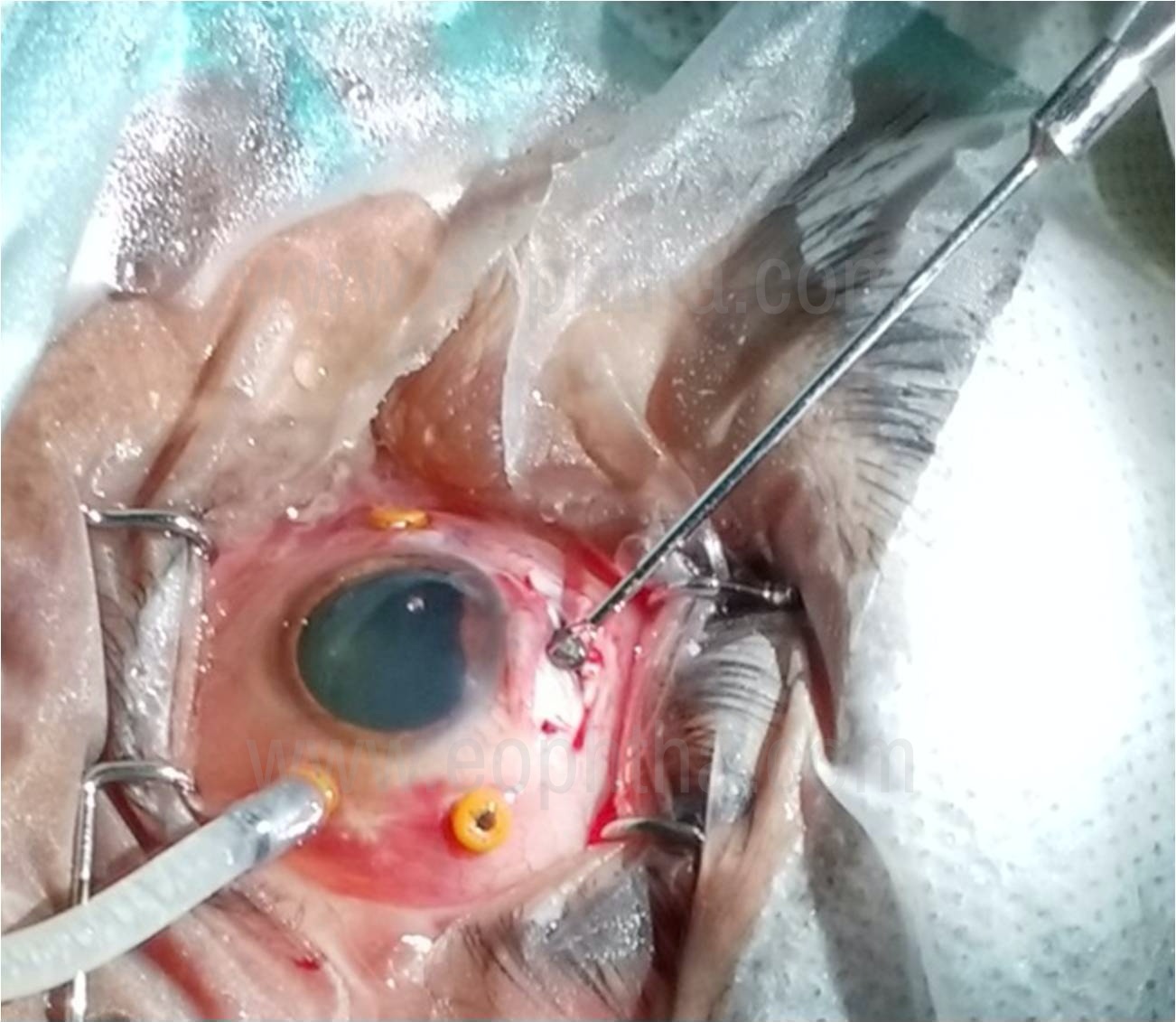
Once the IOFB is released of vitreous attachments, it is lifted from the retinal surface. Various intraocular magnets are available for iron/ ferromagnetic IOFB. Even fairly large IOFB can be lifted using intraocular magnets (Fig.4). For non-magnetic IOFBs, a wide variety of instruments have been described. Various snare devices can be used to hold linear and irregular shaped IOFB. Hikingbotham et al have described diamond-coated forceps6. Acar et al have used basket design forceps device7. This author has described forceps with claw-shaped retractable prongs (Fig.5) that can be effectively used to lift large, irregular, or spherical IOFB from retinal surface8.

Small IOFB can be removed from pre-existing sclerotomy. In the majority of cases, the sclerotomy has to be enlarged to introduce magnet or forceps in the vitreous cavity. Smaller sized IOFBs can be removed through these sclerotomies. However, if IOFB is large or pre-existing sclerotomy has not been enlarged by a surgeon, additional sclerotomy (Fig.6) can be made between superior 2 sclerotomies to remove the IOFB. This approach is useful when the crystalline lens is intact or there is a well centered and stable intraocular lens (IOL) in the visual axis. However, if the patient is aphakic, the surgeon can bring the IOFB in the anterior chamber and it can be removed via a limbal or scleral tunnel. For large or irregular IOFB, the shake-hand technique can be used to firmly grasp the IOFB and orient it along its long axis prior to removal.
(Image Courtesy: Dr. S. Natarajan)
Once the IOFB is removed from the eye, it must be measured and photographed. It should be maintained for medicolegal or academic purposes. Once IOFB has been removed out of the eye, vitrectomy should be completed with the induction of PVD. In cases of IOFBs embedded in retinochoroidal layers, chorioretinectomy can be done after intense endocautery to such areas. Chorioretinectomy is believed to reduce the occurrence of proliferative vitreoretinopathy in the postoperative period. Peripheral retina including sclerotomy sites must be carefully evaluated to rule out retinal breaks or dialysis. Endolaser must be applied around such areas. The choice of tamponading agent depends on case to case basis. In cases where there is no retinal break, no tamponade might be required. While in cases where extensive manipulations are performed, silicone oil is preferred tamponading agent.
Post-operative period
Close follow up is necessary in the postoperative period. Signs of traumatic endophthalmitis or rhegmatogenous retinal detachment must be picked up at the earliest and necessary steps taken. In cases that develop cataract or show its progression after primary surgery require phacoemulsification with IOL implantation. Secondary IOL implantation can be planned in the second stage in aphakic patients. Visual rehabilitation with proper visual aids must be done for all patients.
Conclusion
Open globe injurywith IOFB is usually complex cases that require careful assessment and planning in preoperative period. The Surgeon must have a surgical plan and possible complications in mind. Proper instrumentation like intraocular magnets or various forceps must be kept ready in OR to be used when necessary. Guarded visual prognosis must be explained preoperatively in almost all cases.
References
- Loporchio D, Mukkamala L, Gorukanti K, Zarbin M, Langer P, Bhagat N, et al. Intraocular foreign bodies: A review. Surv Ophthalmol 2016;61:582‑96.
- Fulcher TP, McNab AA, Sullivan TJ. Clinical features and management of intraorbital foreign bodies. Ophthalmology. 2002;109:494-500.
- Modjtahedi BS, Rong A, Bobinski M, McGahan J, Morse LS. Imaging characteristics of intraocular foreign bodies: a comparative study of plain film X-ray, computed tomography, ultrasound, and magnetic resonance imaging. Retina. 2015;35:95-104.
- Williams DF, Mieler WF, Abrams GW, Lewis H. Results and prognostic factors in penetrating ocular injuries with retained intraocular foreign bodies. Ophthalmology. 1988;95:911-916.
- Scott IU, Mccabe CM, Flynn HW, et al. Local anesthesia with intravenous sedation for surgical repair of selected open globe injuries. Am J Ophthalmol. 2002;134:707-711.
- Hickingbotham D, Parel JM, Machemer R. Diamond‑coated all‑purpose foreign‑body forceps. Am J Ophthalmol 1981;91:267‑8.
- Acar N. A new design intraocular foreign body forceps. Retina 2017;37:2378‑80.
- Bapaye M, Shanmugam MP, Sundaram N. The claw: A novel intraocular foreign body removal forceps. Indian J Ophthalmol 2018;66:1845-8.