

Macular Buckling (MB) is simply defined as a modified scleral buckle (SB) surgery where the sclera is remodeled to appose the retina to the sclero-choroidal complex thereby relieving the traction. Unlike conventional SB, where buckle element is placed circumferentially around the eyeball, MB element is placed behind the globe under macula indenting the sclera from posterior. MB has been tried by various surgeons for varied purpose.
In general, situations, where MB has been attempted for a variety of posterior pole diseases, are as follows-
- Eyes with pathological myopia (PM) associated with posterior staphyloma (PS)
- Eyes with Optic Pit abnormalities
- Eyes requiring scleral remodeling posterior to the equator, where routine SB may not be effective
In all practical situations, pathological myopia having posterior staphyloma associated macular changes is presently the most common indications for MB surgery. The other 2 situations have been very rarely attempted with MB surgery, with limited results in the literature.
What are the indications for Macular Buckle surgery?
- Myopic Traction Maculopathy associated with High Myopia and Posterior Staphyloma
- Macular foveoschisis (MS)
- Macular Detachment (MRD)
- Lamellar and/or Full Thickness Macular Hole with MRD
- Failed Vitrectomy for MTM having PS
- Optic pit maculopathy
What’s the Rationale for the considering MB surgery?
The surgical rationale addressing the 3 vector forces acting at macula in a case of MTM with PS, are seen in the schematic diagram.
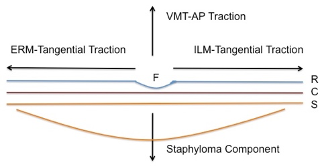
Broadly understanding the mechanism, conventional vitrectomy addresses the anteroposterior traction with PVD separation and ILM peeling or relaxation takes care of the tangential force in majority of the situations . The macular buckle supports the staphyloma area and helps in approximating the retina to the choroidal layer.
In general, the role of MB comes to play when one understands in a given clinical case of MTM, whether vitrectomy alone can help, to consider MB alone or to combined MB with Vitrectomy . In other words, one can choose to perform MB alone or combine with vitrectomy and ILM peeling with tamponade, based on the severity of posterior staphyloma component in a given case of MTM.
For optic disc maculopathy, several mechanisms of pathogenesis have been proposed regarding the possible passage of fluid between the optic nerve sheath and the retinal layers. Hence the rationale of MB in optic disc maculopathy was to abridge or appose the sheath and disconnect the passage, so as to hasten the retinal fluid absorption. MB for these cases have been tried with good long term anatomical success by Theodossiadias et al.1 Technique did not gain its popularity since its introduction 20 years ago because, surgery itself was inherently complicated and also probably better alternatives like more safer microincision vitrectomy. Let the further points henceforth be limited to MTM for the purpose of better understanding.
What is the appropriate timing for planning MB surgery in a given case?
MTMs are chronic and slow progressive pathologies, the majority cases being asymptomatic in nature. Prerequisites for deciding appropriate timing for macular buckle surgery are-
- Recent or new macular symptoms like metamorphopsia, scotoma and/ or reading difficulty, corroborating with changes noted on OCT scans.
- Recent or new progression of macular changes objectively documented on OCT,
In a nutshell, indications of MB surgery is, any MTM changes associated with PS having symptomatic and recent progression of above mentioned macular changes. Chronic and extensive myopic degenerative changes at macula will not benefit functionally with MB surgery.
Are there different types of buckle element and are they commercially available?
Globally , various types of buckle elements have been tried by surgeons. 2 Some are indigenously prepared with locally available clips and sponges. Some are commercially made available to use it directly. Historically, MB using a radially placed polyethylene tube was described for the first time by Charles L Schepens in 1957. Rosengren B (1966), Siam A(1973) and Theodossiadis (1974) have pioneered in using the compatible elements to support macula by various techniques. 3 Some of these techniques have been abandoned due to operative complications.
Some of the commercially available macular buckle are as follows-
- Ando’s Plombe (Ondeko Corp, Japan)4 consists of a semirigid silicone rubber rod, internally reinforced with titanium wires and an indenting head at one end
- T-shaped scleral buckle( FCI, France)5 called as Morin Devin Wedge is created by threading a 4-mm-wide solid silicone ( Devin) band through a 7-mm solid silicone macular wedge (Morin)
- AJL Macular Buckle(AJL Ophthalmic, Spain)2 is custom made PMMA covered by silicone with an indentation area with a spherical helmet in its superior area.
- Adjustable MB ( Micromed Inc, Italy)6 , a silicone rubber radial element, consisting of a “handle” or stalk and a “terminal plate” intended to infold the macula and 2 lateral winglets for suturing. Technique has the possibility of postoperative releasing or augmenting the buckling effect by simply tying temporary knots.
Are the buckles prepared locally?
Macular buckle has also been indigenously prepared by various surgeons since its introduction by Schepens. This non-commercial buckle were broadly made by utilizing commercially available metallic wires and clips, integrating them into sponges thereby fixing them to sclera posteriorly. Mortada from Egypt(2012) used orthodontic steel wire, Siam et al from Egypt (2012) used sponge sutured under direct visualization of post globe surface, Parolini et al from Italy (2015) made an L- Shaped buckle element from a malleable titanium stent (Mod MCP6TP). The techniques, anatomical and visual success of these various buckle surgeries have been compiled in a table in our article for your reference. 3
Are surgical steps the same for any of the macular buckle?
Techniques adopted by various surgeons are different, depending on the buckle element which they have tried in their case series. Broadly, any buckle element would be placed under the staphyloma part and anchored by securing to the sclera in and around the equatorial area of the globe. Need for partial or complete conjunctival opening, the possibility of lateral rectus muscle disinsertion, direct or indirect visualization of macular area (to look for indentation)- were some important parameters which necessitated surgeons to adopt different techniques based on the type of buckle element used. Combining vitrectomy with MB also modified in terms of the order of the surgical steps like buckle placement, scleral securing suture placement, cannula fixation, fluid gas exchange, and tamponade.
We have been using T shaped macular buckle in India, which is also commercially available as ‘Morin Devin Wedge Implant’ and hence we describe the steps of surgery in reference to this buckle element.
Salient surgical steps for Morin Devin T-shaped macular buckle-
- 360° conjunctival peritomy was followed by tagging 4 recti muscles and identification of both obliques.
- The solid silicone macular plate (Morin wedge) was threaded onto the 4mm solid silicone band(Devin Band) to form T shape.
- The Devin band was passed under LR (temporal), inferior oblique, inferior rectus, superior rectus, and superior oblique muscle and brought to the nasal side of the eyeball.
- Macular wedge was slowly maneuvered under the lateral rectus horizontally moving the plate towards the posterior pole.
- Position of the macular plate was checked for correct indentation using wide-angle viewing system under the operating microscope with 25G chandelier placed in pars plana
- The macular plate was secured to sclera under LR. Both ends of the 4mm Devin band was secured to nasal side sclera above and below the medial rectus
- Conjunctiva with the tenons closed meticulously.
How to check the correct indentation?
The position and height of buckle indentation can be checked by-
- IDO examination
- Endo illumination with trocar- chandelier system and wide-angle visualization
- Transillumination with a temporarily fixed 27-G light pipe, cannulated to the buckle element.
What are the surgical difficulties and challenges?
Though not all, some of the surgical techniques of buckle placement described by various surgeons in the literature have certain challenges-
- Lateral Rectus Disinsertion and canthotomy in some of the techniques
- Direct suturing near the macular area is not only challenging, but also has threatening possibility of perforation near macula
What are the complications of macular buckle surgery?
One should keep in mind per-operative, early and late postoperative complications, before contemplating the MB procedure.
Per-operative complications are
- Slippage and misalignment of the buckle element from the macula
- Sudden increase in IOP due to indentation
- Suprachoroidal haemorrhage due to severing of vortex vessels
- Conjunctival buttonholes due to excessive manipulation
Post-operative complications are
- Excessive post-op pain and inflammation( early post-op)
- High IOP( both early and late)
- Subretinal(macular) haemorrhage (early)
- Haemorrhagic Choroidal Detachment( early)
- Misalignment of the buckle position at macula
- Refractive error changes (hypermetropic shift)
- ONH abutting
- Conjunctival erosions and buckle exposure (late)
- Diplopia and motility restrictions (early and late)
What is the take-home message for doing MB surgery?
- Case selection should be very selective based upon clinical examination, OCT findings depicting all maculopathy features in consideration, B-Scan ultrasound for evaluating staphyloma characteristics, wide-angle fundus photographs, Biometry values.
- Recent and fresh macular symptoms which correlate with clinical and OCT changes.
- Should be kept as a reserve option only when conventional vitrectomy procedure may not benefit, in the particular setting, after weighing the pros & cons of the surgery and also it's antecedent complications.
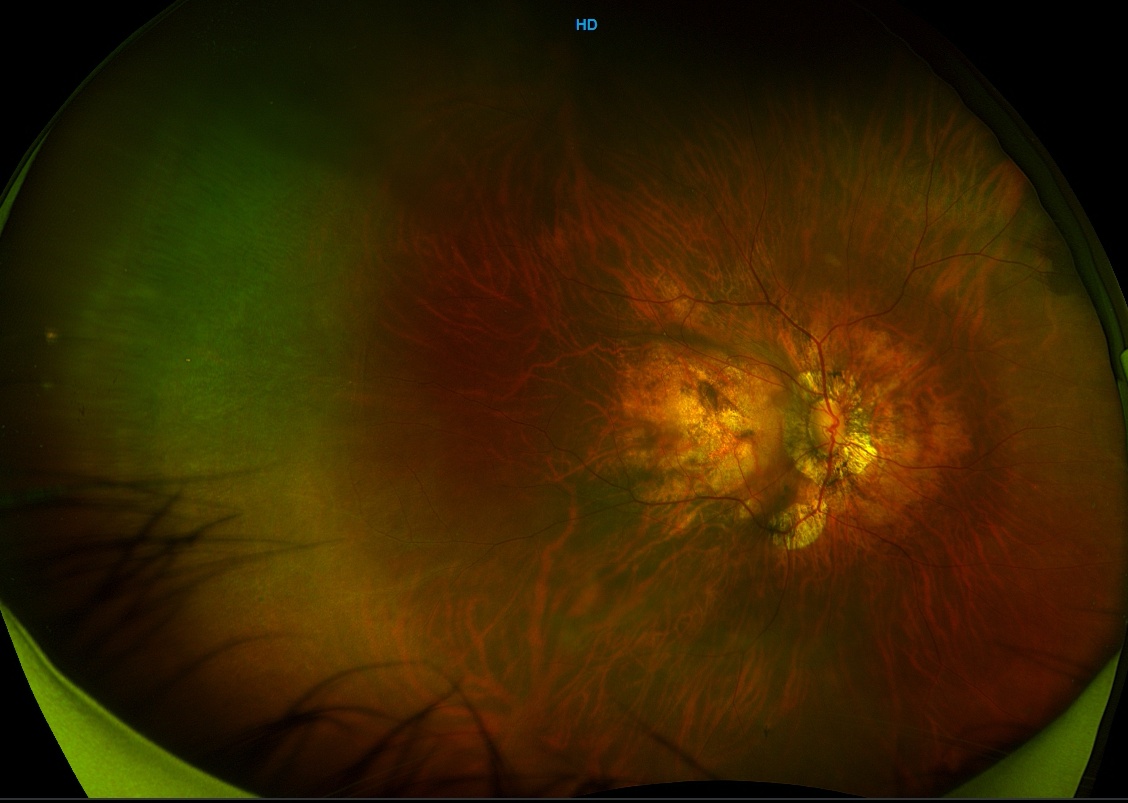
Postoperativefundus photograph of a macular buckle
Suggested reading:
- Theodossiadis GP, Chatziralli IP, Theodossiadis PG Macular buckling in optic disc pit maculopathy in association with the origin of macular elevation: 13-year mean postoperative results. Eur J Ophthalmol (2015); 25:241–248
- Alkabes, M., & Mateo, C. Macular buckle technique in myopic traction maculopathy: a 16-year review of the literature and a comparison with vitreous surgery. Graefe’s Archive for Clinical and Experimental Ophthalmology, 256 (5), 863–877.
- Susvar P, Sood G. Current concepts of macular buckle in myopic traction maculopathy. Indian J Ophthalmol. 2018;66 (12):1772–1784.
- Ando F, Ohba N, Touura K, et al. Anatomical and visual outcomes after episcleral macular buckling compared with those after pars plana vitrectomy for retinal detachment caused by macular hole in highly myopic eyes. Retina 2007;27:37–44.
- Devin F, Tsui I, Morin B, et al. T-shaped scleral buckle for macular detachments in high myopes. Retina. 2011; 31 (1):177-180.
- Cacciamani A., Lazzeri S., Rossi T. et al. Adjustable macular buckling for full-thickness macular hole with foveoschisis in highly myopic eyes: Long-term anatomical and functional results. Retina. 2016; 36 (4): 709-716.