

“The more you know about the past, the better you are prepared for the future.” – Theodore Roosevelt
1. Elicit adequate history
Considering the lethal and angio-invasive nature of Rhino-Orbital-Cerebral-Mucormycosis (ROCM) supplemented in this COVID-19 era, it is mandatory to understand the causative factors of the disease. Diabetes mellitus, oral and systemic corticosteroids, immunosuppressive drugs like tocilizumab, remdesivir, hospital admission, supplemental oxygen, mechanical ventilation, primary or secondary immunodeficiency, hematological malignancies, stem cell transplantation, solid organ malignancies and solid organ transplantation, iron overload etc have been considered the important predisposing factors. The history acts like the guiding lantern onto the path towards appropriate management.
“Ignoring the signs is a good way to end up in the wrong destination”
2. Identify the Red Flag signs
In-depth knowledge about the red flag signs enables the clinicians to recognize the warning signs of ROCM and aids in staging the disease and hence regulate the management. Clinicians need to be alert and must lookout for the signs of ROCM in the COVID-19 survivors during follow-up along with mandatory ophthalmological and otolaryngological examination.
The warning symptoms and signs of ROCM are as follows:
- Nasal stuffiness, Foul smell, Epistaxis
- Nasal discharge - mucoid, purulent, blood-tinged, or black
- Nasal mucosal erythema, inflammation, purple or blue
- Nasal mucosal discoloration, white ulcer, ischemia, or eschar
- Eyelid, periocular or facial edema
- Eyelid, periocular, facial discoloration
- Regional pain – orbit, paranasal sinus, or dental pain
- Facial pain
- Worsening headache
- Proptosis
- Sudden loss of vision
- Facial paresthesia, anesthesia
- Sudden ptosis
- Ocular motility restriction, diplopia
- Facial palsy
- Fever, altered sensorium, paralysis, focal seizures
“Divide and Rule”
3. Categorize ROCM for a systematic approach
ROCM can be categorized as Possible, Probable Proven.
Possible ROCM – Has symptoms and signs of ROCM as mentioned above with concurrent or recent (<6 weeks) COVID-19.
Probable ROCM – Clinical symptoms and signs are supported by diagnostic nasal endoscopy or radiologically by contrast-enhanced MRI or CT scan.
Proven ROCM – Clinico-radiological features along with microbiological confirmation on direct microscopy or culture or histopathology with special stains or molecular diagnostics.
“The best protection is staged detection”
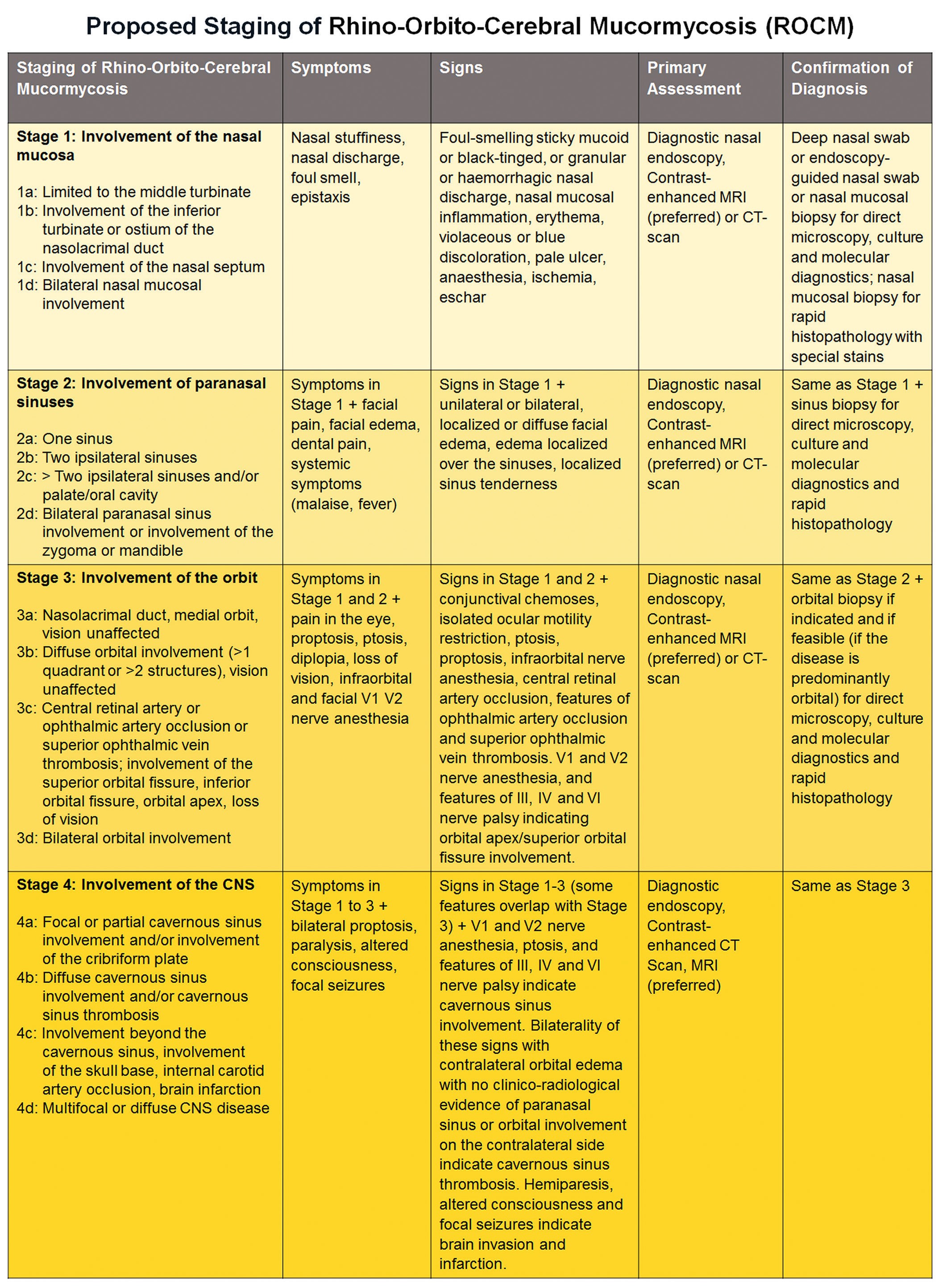
4. Staging of ROCM
The rapid advancement, uncertain predisposition, and unavailability of adequate resources mandate a logical staging of the disease, to timely halt disease progression. This also enables us to streamline the optimal utilization of limited resources in the current pandemic. Figure 1 enlists a proposed staging system. Anatomical progression has been kept as the epicenter of this staging with supplementation of severity.
“Divide and rule, but united we lead”
5. Multi-disciplinary approach
The morbidity and mortality of ROCM can be truncated by a well-woven multi-disciplinary
network of experts in diagnosis (radiology, microbiology, pathology, molecular biology), medical care (infectious disease, neurology, critical care), and surgical care (otorhinolaryngology, ophthalmology, neurosurgery). Appropriate guidelines working in sync with the various disciplines helps in a synergistic management with a holistic approach.
“The most precious resource we have is time”
6. Do not delay
The breakneck speed of progression of this disease does not permit the clinicians to delay in taking the decision for management. A good team of experts must be organized at various levels of healthcare systems. A wholesome approach towards promptly treating the patients with immediate surgical intervention with optimal usage of anti-fungal agents is necessary for the management.
“Desperate times breed desperate measures”
7. Management approach for the stages
Unfortunately, the treatment of ROCM ranges from using only systemic anti-fungal agents to combined extreme surgical interventions. In the early stages, immediate induction of intravenous liposomal Amphotericin B is advocated 5-10mg/kg with strict metabolic control. Less expensive Amphotericin B Deoxycholate (ABDC) or Amphotericin B Lipid Complex (ABLC) are less effective and more toxic alternatives. In cases with impaired renal function IV Isavuconazole 200mg thrice a day on day 1-2, 200mg once a day from day 3; or IV Posaconazole 300mg twice a day on day 1, 300mg once a day from day 2 are recommended.
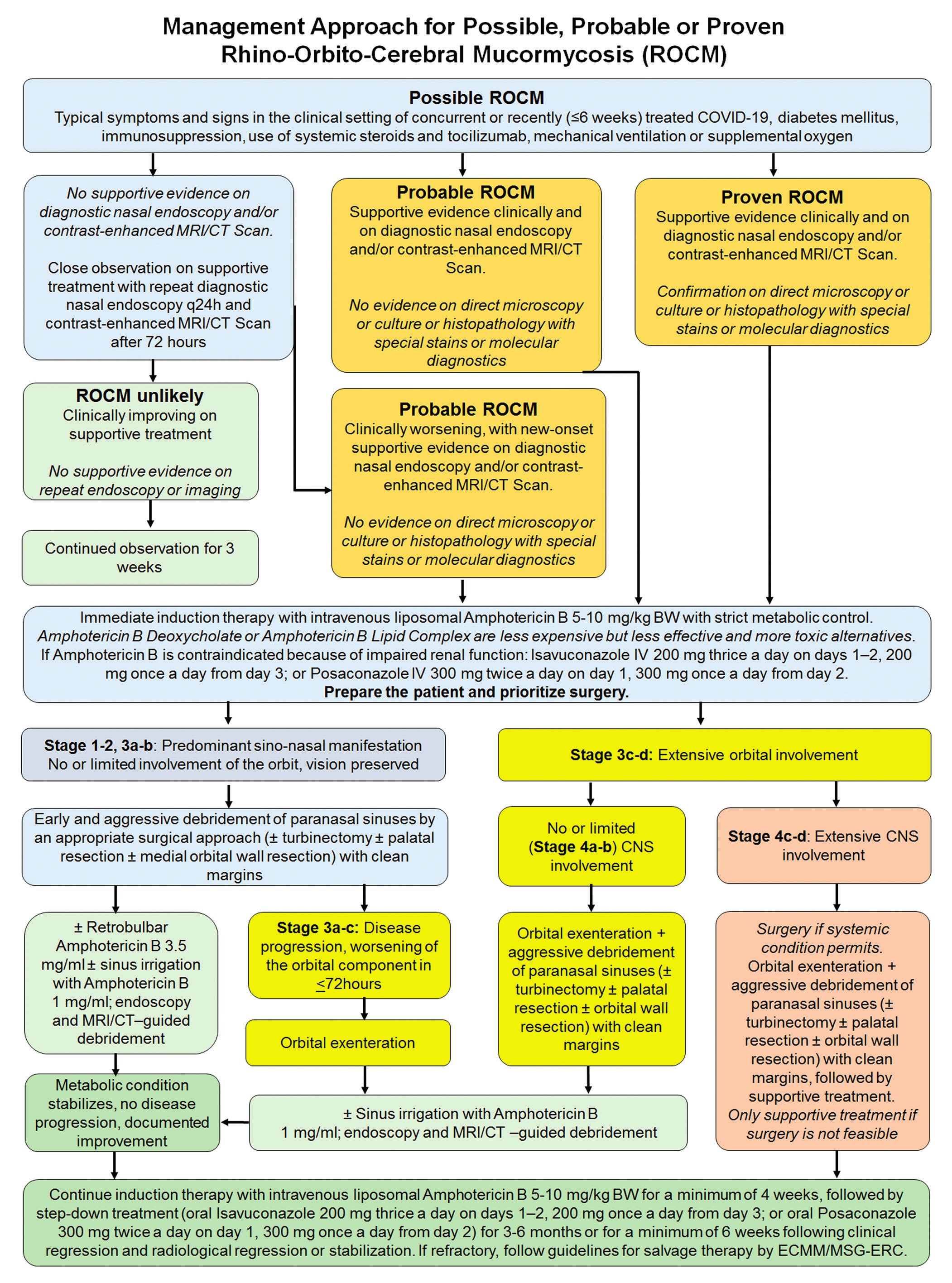
In cases with predominant sino-nasal manifestation, early aggressive debridement of paranasal sinuses with clean margins is mandatory + retrobulbar Amphotericin B 3.5mg/ml + sinus irrigation with Amphotericin B 1mg/ml. Orbital exenteration is performed following paranasal sinus debridement if the orbital component is progressing despite Amphotericin B, or primarily in patients with diffuse orbital involvement at presentation. In cases with extensive CNS involvement, the surgical intervention must be followed by supportive treatment. Continued induction therapy must be implemented for 4 weeks minimum, keeping a check on metabolic status of the patient followed by step-down treatment for 3-6 months or a minimum of 6 weeks following clinical or radiological regression or stabilization
“Quality is remembered long after price is forgotten”
8. Importance of anti-fungal agents
Reasonable yet, liberal usage of anti-fungal agents is required in the management of ROCM. The bigger evil has to be addressed here. However, with the rise in demand, unfortunately, the unavailability of these drugs has posed a barrier for clinicians to be able to wisely treat these patients.
“An ounce of prevention is worth a pound of cure”
9. Prevention of ROCM in the setting of COVID-19
Judicious and supervised use of systemic corticosteroids and tocilizumab in compliance with the current preferred practice guidelines is highly recommended. Nipping ROCM in the bud can be done by aggressive monitoring and control of diabetes mellitus with strict aseptic precautions. We advise excellent personal and environmental hygiene and a barrier mask covering the nose and mouth, and awareness of and due attention to warning signs and symptoms.
“From the ashes, we will rise”
10. Even this shall pass
Even though this rapidly progressive disease has risen from the ashes and has affected the COVID-19 survivors dramatically by increasing morbidity and mortality, a good understanding of disease management and a multidisciplinary approach will help us rise through the devastating consequences of this pandemic. Appropriate and correct awareness regarding the disease red flag signs can promote early detection and avoid unnecessary panic. A protocol based-strategy with a meticulous multi-disciplinary team with a prioritized approach is the way to find the light even in the darkest places.