.jpg)
As like other strabismus, esodeviation can be,
- True esodeviation
- Pseudo esodeviation
- A prominent epicanthic folds 1, 2
- Negative angle kappa in high myopes.
True esodeviation can be either comitant or incomitant 1,2
A. Comitant
I. Accommodative esotropia.
- Refractive accommodative esotropia (normal AC/A ratio)
- Non Refractive accommodative esotropia (high AC/A ratio)
- Hypo accommodative esotropia (reduced NPA)
Partially accommodative esotropia
II.Non-accommodative esotropia
- Essential infantile esotropia
- Non-accommodative convergence excess
- Acquired esotropia
- Acute Onset esotropia
- Divergence insufficiency or paralysis
- Cyclic esotropia
- Recurrent esotropia
III. Microtropia
IV. Nystagmus blockade syndrome.
B. Incomitant
Paralytic- Neurogenic (VI nerve palsy)
Nonparalytic- Myogenic (ocular myasthenia)
-
-
- A & V pattern syndromes
- Duane’s retraction syndrome
- Mechanical – restrictive esodeviation
- Congenital fibrosis syndrome
- Acquired
- Dysthyroid eye disease
- Trauma to the orbital wall
- Myositis (IOID)
CONGENITAL ESOTROPIA:
Essential infantile esotropia was initially called congenital esotropia. But former term preferable as term essential explains the unknown etiology and ‘infantile’ the period of occurrence. The esodeviation is rarely present at birth to term it congenital. Esodeviation persisting at >4months of age is considered to be abnormal 3,4.
Features include1, 3
- age of presents < 6 months
- Large, constant the deviation (> 30PD)
- Initial alternation with cross fixation
- Asymmetric OKN (Naso-temporal asymmetry of OKN persists)
- Absence of neurological deficits.
Other findings which may be present include,
- Inferior oblique overaction (68% of cases)
- Manifest – latent nystagmus
- DVD (dissociated vertical deviation)
- Amblyopia
- Apparent limitation of abduction
- Further deviation not attributable to refractive error.
Ocular movements have to be noted in infants by the doll’s head manoeuvre or rotation test.
Management:
1) Treat amblyopia by conventional patching 1,3,4
2) Surgery :
Timing of the surgery -
Very early surgery ( within 6 months) Vs Early surgery (6 months -2 years ) Vs late surgery (2.5 – 5 years) 11-14
Very early surgery has the advantage of restoring binocular function. Few advocate surgery as early by 2 months but Helveston etal suggests surgery by 4 mon of age.
- Wright etal., showed high-grade stereopsis could be obtained in some patients with surgery between 13 and 19 weeks of age.Further subset of patients operated at 4 months gained fine grade stereopsis in 60 % of them
- Regaining stereopsis and reversal of motion VEP asymmetry were higher in this group but with problems of need for repeat surgeries
With regards to early surgery ( 6 months -2 years ) ;
Meta-analysis showed sensory results are better if the good alignment is obtained prior to 24 months of age as opposed to later; however, it found no difference in outcomes if the alignment was obtained by 6 months, 12 months, or prior to 24 months of age, respectively. And thus gives the optimum of operating early with consistent results
Late surgery has poor results with respect to stereopsis. ELISSS - Early Vs late infantile strabismus surgery study showed that children operated early had better gross stereopsis at age 6 as compared to those who are operated late.
Surgical plan:
Bimedial recessions preferred with measurements from limbus because of the variable distance of insertion of medial rectus from in limbus in infancy. Unilateral surgery is preferred in amblyopic eyes. DVD may manifest following initial surgery and needs to be managed.
Subnormal binocularity is the optimal goal. But usually, the surgeon has to be satisfied with a Microtropia( central suppression with peripheral fusion) or a small residual esotropia.
Botox injections into medial rectus also tried with variable results.
Differential diagnosis includes:
- Infantile accommodative ET
- Congenital VI nerve palsy
- Duane’s retraction syndrome.
- Moebius syndrome
- Congenital myasthenia
- Congenital fibrosis syndrome
Other syndromes:
Ciancia syndrome: Includes patients C essential infantile esotropia, latent nystagmus, head turn towards the adducting eye, and apparently limited abduction in both eyes.
Lang syndrome: the term used for the association of infantile ET, DVD & abnormalhead posture(head tilt)
ACCOMMODATIVE ESOTROPIA
An esotropia caused by an increased accommodative effort or an abnormally high AC/A ratio is referred to as accommodative esotropia1,2,5.
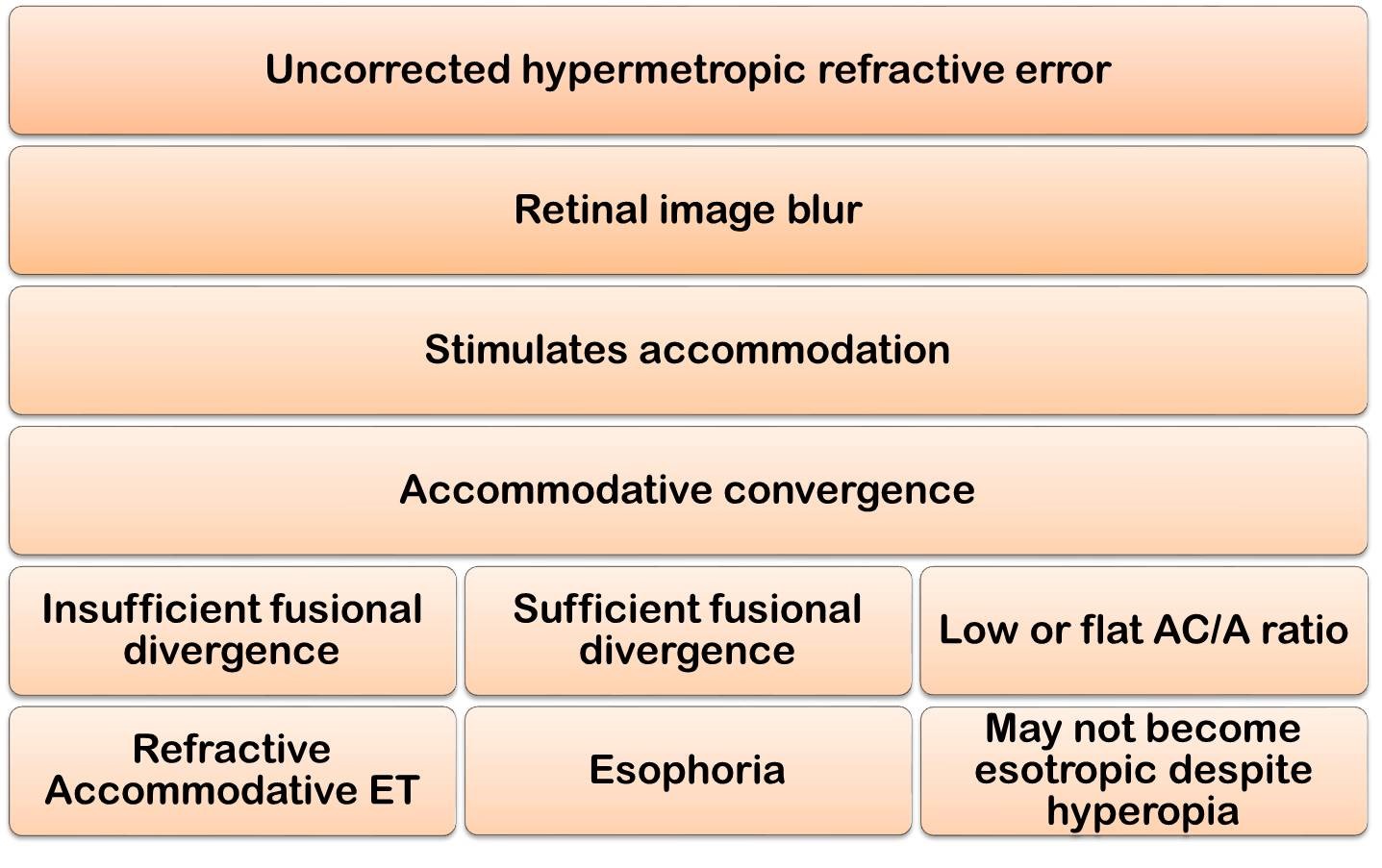
The above flow chart explains why few children with hyperopia develop esotropia & others don’t.
Refractive accommodative esotropia:
Characteristics: Onset of 1 – 3 years. (the exception being infantile-onset accommodative esotropia which occurs in < 1 year of age.)
- Variable angle usually between 15 to 40 pd.
- Intermittent deviation
The most important step diagnosis of accommodative ET is proper cycloplegic refraction. Adequate cyloplegia is obtained after 30 – 40 min of instillation of 2 drops of 1% cyclopentolate (5 min apart) 0.5% in children < 6 mon of age) 62.
Atropine Vs cyclopentolate
|
Atropine |
Cyclopentolate |
|
|
Second important thing is to rule out the presence of a high AC/A ratio. Clinically when the deviation (ET) at near more than the distance by 10-15pd, high AC/A is indicated.AC/A can further be quantified using the heterophoria method or lens gradient method, the latter being superior than the heterophoria method. High AC/A ratio means that there is higher accommodative convergence than normal for each dioptre of accommodation with a normal near point of accommodation.
Treatment:
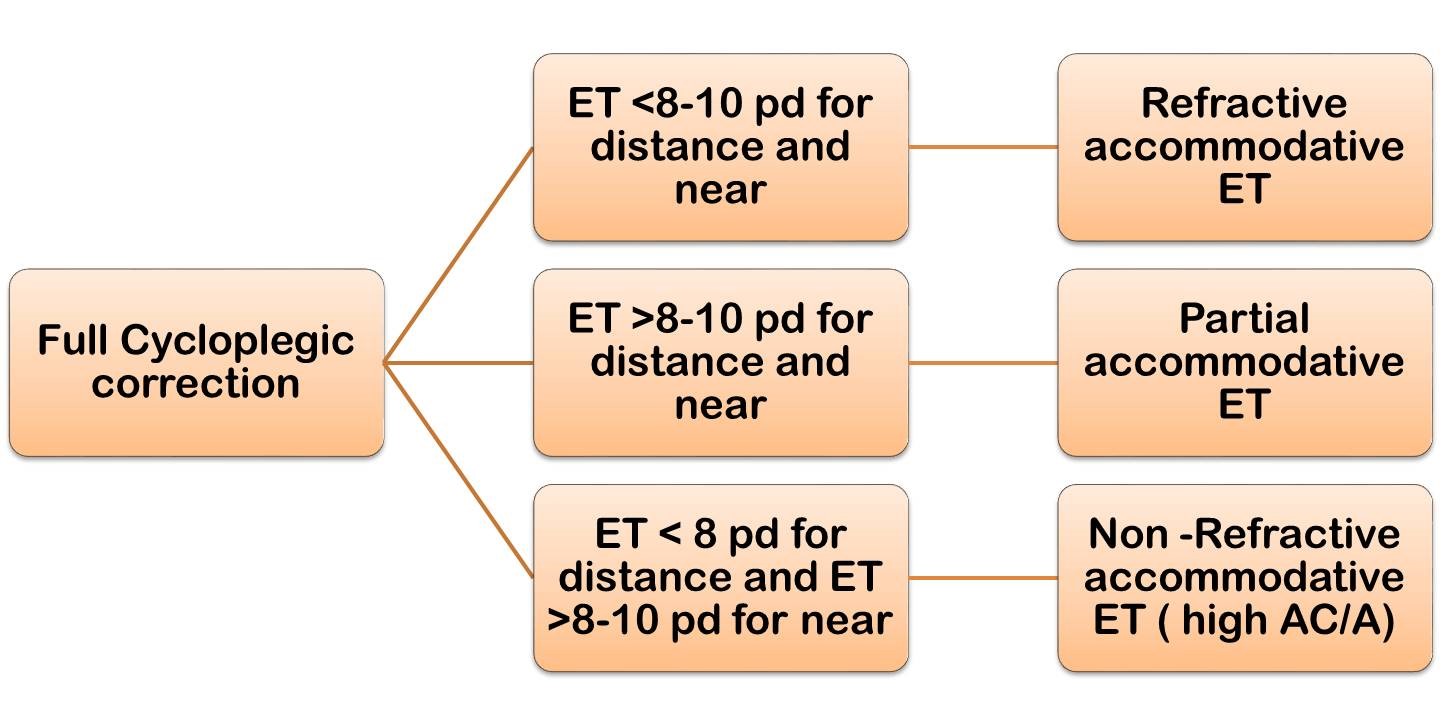
The basic cause in refractive accommodative ET is the presence of uncorrected hypermetropia, thus correcting refractive error forms the mainstream of management.
- Full cycloplegic correction needs to be prescribed, i.e. without deducting for cycloplegic value of cycloplegic agent. Glasses are to be worn full time. In children who have difficulty in relaxing accommodation and thus in accepting correction, short course of cycloplegics (atropine or cyclopentolate) is given.
- With time full correction, if the deviation is reduced to within 8 pd, it is refractive accommodative ET and nothing further needs to be done.
- If the deviation is within 8 PD for distance but more than 10 PD for near, it is suggestive of high AC/A ratio. It is called Non-refractive accommodative esotropia . Such case necessitates the use of bifocals. The bifocals relieve the accommodation, thus maintain alignment for near & provide binocularity. The best bifocals are flat top executive bifocals that bisect the pupil. An add +2.500 to 3.00D is usually required. The minimum add which can be prescribed is +1.25 D
- Child can usually be weaned off bifocals by 9-10 years of age.
- Anticholinesterase agents are an alternative method of facilitating accommodative efforts. These drugs inhibit cholinesterase enzyme at neuromuscular junction, thus Ach released at ciliary body stays longer. So, small accommodative effort results in large amount of accommodation, (called peripheral accommodation). Examples include 0.03 – 0.125% echothiophate iodide topically.
Side effects include,
- Ocular – iris cysts along pupillary margin. Use of phenylephrine prevents cyst formation.
- Systemic : Browaches, nausea, abdominal cramps.
- Prolongs action of succinyl choline, thus latter anaesthetic not to be used if child was on miotics with in 6 weeks prior to surgery.
- If with full correction, deviation persists both for distance and near and is more than 10 pd, it is called partially accommodative esotropia. Surgery for the residual deviation is the treatment of choice. Amount of surgery to be done is controversial. Using average of near and distance deviation as target angle results in 25% under correction.
- Average of near deviation with and without correction glasses as a target angle reduces the number of under correction. Further, the average of DD with correction and ND without correction may be prudent in those with associated high AC/A ratio.1,2,7.
Prism adaptation before surgery is advocated by a few surgeons 8.
Non-accommodative convergence excess esotropia (Normal AC /A ratio)
Esotropia is larger at near (at least 154) than at distance1,2 AC/A is normal with normal NPA, unlike hypoaccomodative esotropia. These patientsdo not benefit from bifocals or miotics. Surgery is required to align them and preserve binocularity but has varied results.
Divergence insufficiency or paralysis. 1,2,9
Usually occurs in elderly patients. Pt complains homonymous diplopia for distance. Esotropia which is greater for distance than near, almost orthotropic for near. Fusional divergence amplitudes decreased both for distance and near. This is considered to be a distinct entity & different from B/L 6th nerve palsy. Usually, conditions causing increased intracranial pressure, intracranial tumours, head trauma & vascular lesions of the brain stem may be associated with divergence paralysis.
Cyclic Esotropia 1, 10
Refers to unique esotropia which follows a 48 hrs rhythm, i.e. a 24 hrs period of normal binocular vision followed by 24 hrs of manifest tropia.
- It usually becomes apparent during early childhood.
- On ‘Straight days’ no anomalies of binocular vision are observed (no phoria also).
- On ‘strabismus days’, a large angle esotropia often as large as 40pd– 50pd will appear. Sensory anomalies like fusional amplitudes are defective on these days.
- Cyclic nature may last for a month to years, after which it breaks & esotropia becomes constant.
- Surgery for deviation measured on ‘squint days’ gives satisfactory results.
Sensory esotropia 1,2
Esotropia which occurs secondary to unilateral vision loss is termed sensory esotropia. Vision loss in children aged < 2 – 4 years results in esotropia, whereas in older children causes sensory exotropia. Surgery usually confined to the blind eye in such cases.
Nystagmus blockade syndrome 1, 2
Patients with congenital nystagmus and straight eyes may use convergence to dampen nystagmus which may result in esotropia. There is an inverse relation between nystagmus and esodeviation. i.e. when the patient is ortho nystagmus intensity is maximum; with the onset of esotropia, nystagmus dampens. Surgery in excess of routine MR recession is usually needed in such cases.
Consecutive Esotropia:
Esotropia following surgery for exotropia is termed consecutive esotropia.
If the question asked is, write on DD and management of a Six-month-old child presenting with esotropia?
The DD includes Infantile accommodative ET
- Congenital VI nerve palsy
- Duane’s retraction syndrome
- Infantile accommodative esotropia
- Moebius syndrome
- Congenital myasthenia
- Congenital fibrosis syndrome
If asked on, Write on DD and management of 3-4-year-old child presenting with esotropia?
Write on
- Refractive accommodative ET
- DRS type I or Esotropic DRS
- Cyclic ET, Sensory ET
- VI nerve palsy, ET associated With Down’s syndrome, CNS disorders, and others
References:
- Von Noorden GK. Binocular Vision and ocular motility. St. Louis : CV Mosby; 1996: pg 437 – 442.
- Kenneth W wright. Pediatric Ophthalmology and strabismus Mosby; 1995 : pg 179 – 195
- Helveston, EM. Frank contenbader lecture – the origins of congenital esotropia. J Pediatr Ophthalmol strabismus 30; 215: 1993
- Noorden G.K. Von. Current concept of infantile esotropia Eye 2:243, 1988.
- Noorden GK Von, Avilla CW : Accomodative convergence in hypermetropia. Am j ophthalmol 110; 287, 1990.
- Abraham Sr: The use of echothiophate – phenylephrine formation in the treatment of convergence strabismus and amblyopia with special emphasis on iris cysts. J Pediatr Ophthalmol strabismus 1: 68, 1964.
- Wright KW, Bruce Lyle L : Augmented surgery for esotropia associated with high hypermetropia. J Pediatr Ophthalmol strabismus 30: 167-170, 1993.
- Prism adaptation research group: Efficacy of prism adaptation in surgical management of acquired esotropia. Arch Ophthalmol 108 : 1248 – 1256, 1990.
- Bielschowsky A: Lectures on motor anomalies of the eye Arch Ophthalmol 1935; 13:580.
- Caputo AR, Greenfield PS : cyclic esotropia. Ann Ophthalmol 1978; 10: 775.
- Wright KW, Edelman PM, McVey JH, Terry AP,Lin M. High-grade stereo acuity after early surgery for congenital esotropia. Arch Ophthalmol. 1994;112:913–9.
- Ing MR. Early surgical correction for congenital esotropia. J Pediatr Ophthalmol Strabismus. 1983;20:11–8.
- Ing MR. Outcome study of surgical alignment before six months of age for congenital esotropia. Ophthalmology. 1995;102:2041–5.
- Simonsz HJ et al. Final report of the early Vs late infantile strabismus surgery study(ELISSS),a controlled ,prospective multicenter study.strabismus.2005