

Introduction:
Macular edema is defined as swelling of the layers of neurosensory retina within the macula. Cystoid macular edema (CME) is a subtype of macular edema characterized by extracellular accumulation of fluid within the outer plexiform layer of the retina in the form of intraretinal cyst. It is known as one of the complications, that develops consequent to a final common pathway in diverse diseases affecting the blood-retinal barrier.
CME is a major cause of visual loss in uveitis. The overall reported prevalence of visual impairment associated with uveitic CME is 33–42 % and is influenced by the age, location, severity, and duration of retinal edema. [1,2] In young age, the retinal tissue shows resistance to development of CME, but advanced age is independently associated with early development of CME, regardless of the duration of uveitis. In contrast, the most frequent causes of visual loss in pediatric uveitis are retinal scars and glaucoma. [3] Panuveitis and intermediate uveitis are responsible for 50% and 40% of visual impairment due to CME respectively. [2] (Table 1) Concurrent presence of systemic cardiovascular disease with intraocular inflammation predispose to early development of CME. [4] Smoking and microalbuminuria appear to have a greater prevalence of CME in uveitis patients.[5]
|
Table 1: Causes of Inflammatory CME |
|
|
Panuveitis Vogt-Koyanagi-Harada disease Sympathetic ophthalmia Endophthalmitis Sarcoidosis Adamantiades-Behçet disease Multifocal choroiditis and Panuveitis Immune recovery Uveitis SLE-related panuveitis Idiopathic panuveitis Posterior Uveitis Toxoplasmosis CMV Retinitis Birdshot retinochoroidopathy Acute Retinal Necrosis Retinal vasculitis |
Intermediate uveitis Pars planitis Associated with multiple sclerosis Anterior uveitis Idiopathic HLA-B27 associated Juvenile Idiopathic Arthritis Miscellaneous Trauma Intraocular surgery Intraocular lymphoma Drugs (Prostaglandin analogues, nicotinic acid, zidovudine, rifabutin) |
Pathogenesis
In physiologic conditions, the retina maintains a transparent and relatively dehydrated state due to a balance between fluid entry and fluid exit in the tissue. Fluid enters the retina from the vitreous, the retinal vessels and exits from the subretinal space through the retinal pigment epithelium (RPE) into the choroid and the retinal Müller glial cells back into the retinal vessels. This dynamic process is controlled by the inner blood-retinal barrier (BRB) formed by the endothelial tight junctions, pericytes, astrocytes, and Müller cells and the outer blood-retinal barrier formed by the tight junctions of the RPE. An imbalance in this entry-exit process leads to accumulation of fluid within and/or under the neurosensory retina. The pathogenesis of inflammatory CME is yet not fully understood and an interplay of various mechanism might contribute to its development.
A. Vasogenic Mechanism
CME develops the following disruption to the BRB. Intraocular inflammation causes cellular damage resulting in activation of the arachidonic acid cascade and release of prostaglandins (PGE), nitric oxide (NO), interleukin 6 (IL-6), and vascular endothelial growth factor (VEGF).[6-8] These inflammatory mediators have been identified in the aqueous humor of patients with active uveitis leading to a pathologic hyperpermeability of the retinal vessel walls and causing damage to the RPE, resulting in fluid and protein extravasation into the retinal interstitium.[8] The RPE dysfunction contribute to reduced pumping of fluid into the choroid and rather fluid entry from the choroid to the subretinal space. Smoking and coexistent vascular disease also play a role in the pathogenesis of inflammatory macular edema
B. Cytotoxic mechanism
Müller cells in the retina play a role in absorbing water from the retinal tissue by water transport coupled to the potassium clearance function. Pathologic conditions increase the conductance of potassium into the Müller cells and intracellular swelling. Intraretinal cyst, in part result from Müller cell swelling and necrotic death. Also, these cells flux water in and out of the retinal vessels through AQP4 channels, which is also altered in inflammation conditions. [9]
C. Morphological mechanism
Intraocular inflammation heralds the induction of posterior vitreous detachment in eyes. When mechanical tractional forces are exerted at the vitreoretinal interface by partial vitreous detachment, it can augment formation of macular edema. Traction on internal limiting membrane (ILM) which is formed by the intertwined foot processes of Müller cells, can cause irritation of the cells and result in the local release of inflammatory mediators. Mechanical pull over the retinal vessels located at the inner retina by the detaching posterior hyaloid, may deform and alter vascular walls with subsequent leakage. Also, persistent tractional forces may lead to decreased interstitial hydrostatic pressure, resulting in increased flux of fluid from the vascular compartment. [9]
Clinical Picture
The most common clinical manifestation of macular edema is a reduction in central visual acuity. Reading acuity and reading speed are good indicators of functional impairment of vision. [10] Contrast sensitivity reduction and impaired colour vision can contribute to the functional visual impairment. However, edema may exist without impairing visual acuity, only to be detected on retinal imaging. It is not sufficient to rely on visual acuity to exclude the presence of macular edema or resolution of edema in response to treatment. Micropsia is often another clinical manifestation, in which objects appear smaller than they really are due to increased separation between photoreceptors by the accumulated fluid. This may give rise to metamorphopsia as well.
The formation of fluid-filled cysts in a petaloid fashion is clinically observed by slit-lamp biomicroscopy. It may be concurrently associated with epiretinal membrane or vitreo-macular traction. But sometimes, early changes may go unnoticed on clinical examination despite using 78D or 90D indirect lenses. With the advent of new diagnostic instrumentation like Fluorescein Angiography (FA) and Optical Coherence tomography (OCT), even subtle changes in retinal thickness can now be detected.
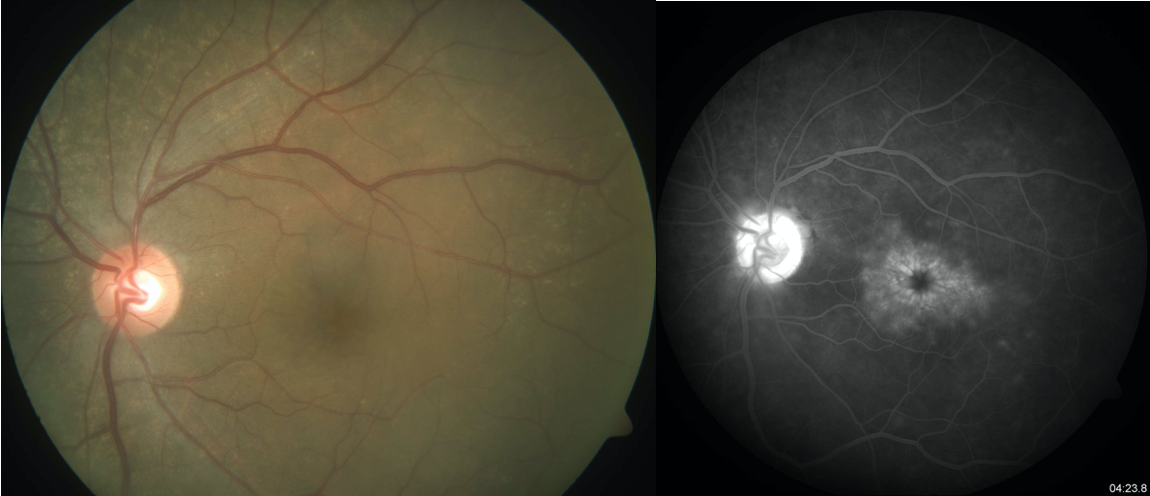
Figure 1: Fundus photograph of a patient with cystoid macular edema. FFA of the same eye showing flower-petal appearance.
Ancillary investigations
Early detection of cystoid macular edema is critical for diagnosis and management. Traditional methods of accessing macular edema include contact and non-contact slit-lamp biomicroscopy, indirect ophthalmoscopy, fluorescein angiography, and fundus stereo photography. The use of OCT has improved our understanding of CME. (Table 2)
Fluorescein angiography
Fluorescein angiography is an invasive technique that confirms the presence of CME in intraocular inflammation qualitatively. In the early phase of the angiogram, capillary dilation is seen in the perifoveal region. Late phases show the pooling of the dye into the fusiform cystoid spaces. These spaces are arranged radially in the perifovea giving rise to petaloid pattern, owing to the oblique arrangement of fibers in the outer plexiform layer (OPL). When cystoid spaces occur outside the perifoveal area, fluorescein angiography shows a ‘honeycomb’ appearance rather than a petaloid pattern, due to the vertical arrangement of OPL fibers. Often patchy hyperfluorescence is seen extending beyond the region of the cystic spaces indicating more widespread capillary leakage. Leakage of the dye from the disc capillaries gives rise to the late staining of the optic nerve head. In addition to the presence of leakage, it also provides information about the perfusion state and foveal avascular zone abnormalities. However, poor quantification of retinal thickness has allowed OCT to supersede fluorescein angiography for CME.
Optical Coherence Tomography
OCT is a non-invasive imaging modality providing near histological resolution of retinal layers. It can quantify CME by its ability to measure the thickness of the retinal tissue. OCT can help in the detection of early edema and monitoring the treatment efficacy, especially when vitreous cells are present in uveitis. CME on OCT shows the extent of retinal thickening and the retinal layer involved, appearing as nonreflective cystoid spaces in the outer plexiform and inner nuclear layers. OCT patterns have been identified in CME associated with uveitis: diffuse macular edema (characterized by increased retinal thickness, disturbance of the layered retinal structure or sponge-like low reflective areas); cystoid macular edema (characterized by clearly defined intraretinal cystoid spaces) and serous retinal detachment (characterized by a clean separation of the neurosensory retina from the RPE/choriocapillaris band). OCT also detects Epiretinal Membrane (ERM), vitreo-macular traction (VMT), and choroidal neovascular membrane associated with uveitis. OCT is now the preferred non-invasive imaging, making it patient-friendly during frequent follow-up visits to monitor changes.
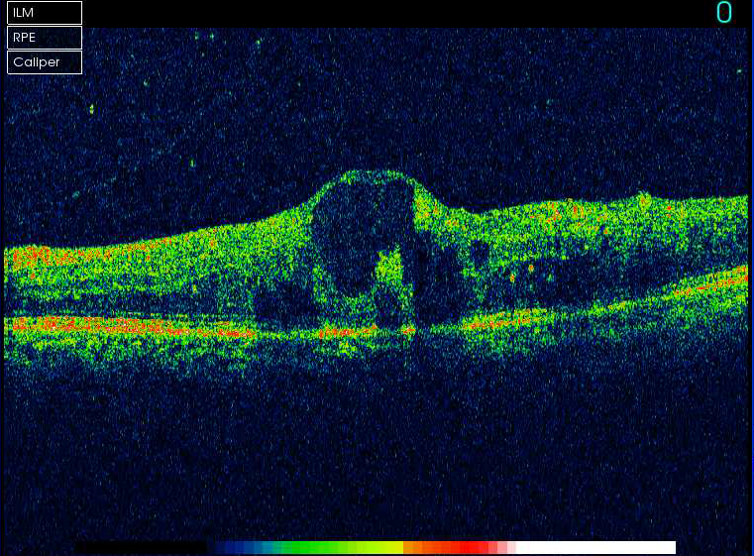
Figure 2: OCT showing cystoid macular edema
|
Table 2: Fluorescein Angiography & Optical Coherence Tomography in inflammatory CME |
||
|
Features |
FA |
OCT |
|
Technique |
Invasive |
Non-invasive |
|
Principle |
Fluorescence |
Low coherence interferometry |
|
Dye |
Sodium fluorescein |
No dye used |
|
Information |
Qualitative (Location and extent of leakage) |
Both qualitative and quantitative (Location and thickness measurement) |
|
Assessment |
Subjective |
Objective |
|
Images analysis |
Dynamic study of sequential images |
Study of static images |
|
Measure Retinal thickness |
No |
Yes |
|
Retinal Perfusion |
Yes |
No |
|
Vitreo-retinal interface abnormalities |
Not detected |
Detected |
|
Adverse reactions |
Associated with dye |
Absent |
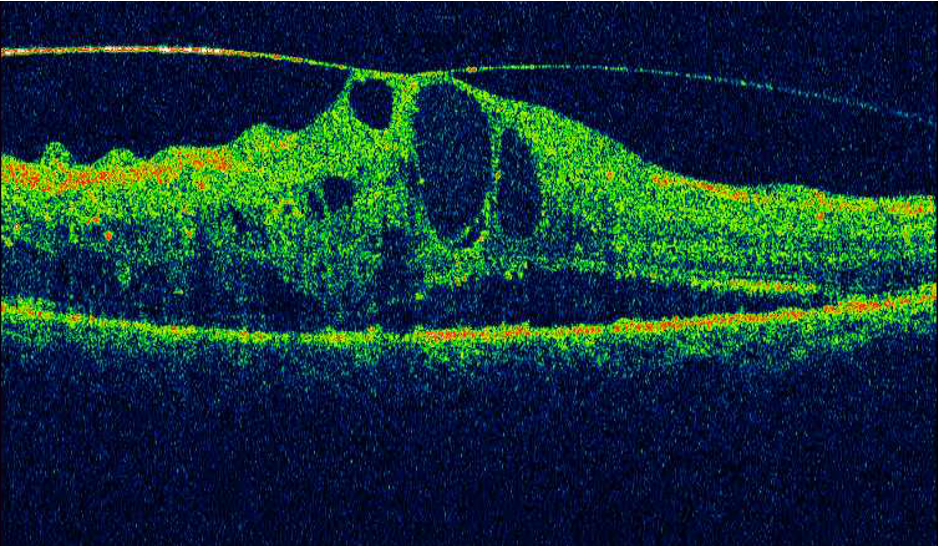
Figure 3: OCT showing CME with VMT
Complications
Chronic CME is defined as a decrease in visual acuity with increased retinal thickness and intraretinal cysts by OCT and/or leakage on fluorescein angiogram for 6 months or more. The edema becomes recalcitrant when it fails to resolve despite multiple therapies. This leads to cysts, macular (pseudo) hole, macular ischemia, permanent photoreceptor damage, retinal atrophy, and fibrosis, such that normal vision may not return even after the resolution of edema. Nonetheless, restoring the normal architecture of the retina without restoring normal vision, has a better prognosis for maintaining visual acuity.[2] And for these reasons, any amount of CME warrants treatment until its disappearance.
Treatment
The decisive mechanisms involved in the development and persistence of uveitic CME have not been established yet. So, the treatment options are mainly directed toward limiting the inflammation through anti-inflammatory agents and removing toxic mediators from the vitreous. The principles of treatment for inflammatory CME include treatment of the underlying disease, symptomatic medical management, less often surgical interventions and lifestyle modifications (smoking cessation for patients with uveitis) [11]
The medical treatment possibilities include identifying and treating the underlying infectious agent (toxoplasmosis, CMV retinitis), anti-inflammatory drugs and carbonic anhydrase inhibitors. Recently anti-vascular endothelial growth factor (VEGF) drugs, immunosuppressives, biologics and somatostatin analogs have been added to the armamentarium. (Table 3) The surgical option of pars plana vitrectomy is aimed at release of traction and removal of possible toxic mediators in the vitreous. The definite choice of local and/or systemic treatment modalities for macular edema is influenced by the severity and laterality of the disease.
|
Table 3: Treatment agents for CME |
|
|
Systemic therapy |
Local therapy |
|
Corticosteroids |
Corticosteroids (Topical, Periocular, Intravitreal) |
|
Immunosuppressives |
Topical Nonsteroidal anti-inflammatory drugs (NSAIDs) |
|
Biologics |
Intravitreal anti-VEGFs |
|
Carbonic anhydrase inhibitors |
|
Nonsteroidal anti-inflammatory drugs (NSAIDs)
NSAIDs block cyclooxygenase enzymes and inhibit prostaglandin synthesis to reduce inflammation. Topical Indomethacin (0.5%) has shown to improve inflammatory macular edema at 6 months follow-up in a double-blind, placebo-controlled randomized prospective trial.[12] Topical Bromofenac has better ocular penetration and synergistically reduces edema along with intravitreal steroids.[13] The efficacy of oral NSAIDs have not been reported for uveitic CME. Although NSAIDs are regularly prescribed for inflammatory macular edema, their efficacy is disappointing.
Corticosteroids
Corticosteroids remain the mainstay for the treatment of vision-threatening uveitis owing to their rapid onset of action. They possess anti-inflammatory properties that down-regulate cell adhesion and transmigration, suppress the synthesis of prostaglandins and leukotrienes, inhibit cytokines (IL-6, TNF-alpha, VEGF) production, and stabilize the blood-retinal barrier by decreasing the vaso-permeability. There are various routes of administration viz. oral, topical, periocular, intravitreal, or steroid implant. The aim of the therapy is to achieve the highest intraocular concentration with minimal side effects.
Topical Corticosteroids
Topical corticosteroids are the easiest form of local therapy and its use is often limited for anterior segment inflammation due to poor ocular penetration. Difluprednate 0.05% has superior penetration as compared to other available agents. But it runs a risk of cataract development and intraocular pressure (IOP) elevation, especially in children, and requires close monitoring.
Systemic Corticosteroids
Oral prednisone is rapidly absorbed and reaches a peak concentration of 30 minutes to 2 hours after ingestion. Owing to this, it is indicated in the treatment of vision-threatening bilateral uveitis with inflammatory macular edema or that refractory to topical treatment. The recommended induction dose is high (1mg/kg/day, maximum adult dose 60-80 mg/day) to achieve rapid anatomical recovery of the macula. [14] Their long-term use, however, is not recommended due to serious potential side effects, which include peptic ulceration, osteoporosis, aseptic necrosis of the hip, weight gain, Cushing syndrome, muscle weakness, hyperglycemia, systemic hypertension, the progression of glaucoma and cataract. The patient needs appropriate counseling regarding the side effects, against the abrupt stopping of drugs and avoidance of pregnancy and breastfeeding. If the intraocular inflammation fails to maintain remission with less than 10 mg/day or equivalent by 3 months, alternate therapy with immunosuppressives should be considered.
Periocular Corticosteroids
The rationale of periocular injection is the ability to deliver a high concentration of drug within close proximity to the macula. They are indicated in unilateral disease or as adjuncts to systemic treatment for refractory uveitic macular edema. The common methods used to administer are posterior subtenon or orbital floor injections of triamcinolone acetonide. The posterior subtenon injection in the superotemporal quadrant (Nozik’s technique) is advocated in the management of CME. [15] Ultrasound studies have shown that the drug injected through this route takes retromacular position, from where it diffuses in the eye trans-sclerally. The effect the drug in resolution of edema lasts anywhere between 3-6 months and usually require serial injections in unresponsive patients. Repeated injections are commonly associated with ptosis, elevated IOP and cataract progression. Rarely devastating complications like globe perforation, optic nerve injuries, retinal detachment, and vascular occlusion may occur.
Intravitreal Corticosteroids
Intravitreal corticosteroid is a direct local therapy that reduces intraocular inflammation at the site, without adverse systemic side effects. It bypasses the blood-retinal barrier, leading to a more concentrated dose of steroids into the vitreous cavity for a prolonged period. Triamcinolone acetonide(TA), a water-insoluble synthetic steroid, is commonly injected in a dose of 4mg/0.1ml. It has a response as early as 1 week, a peak response in 4-6 weeks, and effect lasts between 6 week to 6 months. Many patients require multiple injections to maintain improvement in visual acuity and intraocular inflammation, especially old age with chronic edema. This further increases their risk of IOP elevation, development of posterior subcapsular cataract, with the added risk of endophthalmitis with multiple injections. Preserved TA containing benzyl alcohol as a preservative, is presumed to cause non-infectious (sterile) endophthalmitis and has an off-label intraocular use.[16] The development of sterile, preservative-free preparation of TA is designed for intraocular use and FDA approved for intraocular inflammation. However, the side effect profile of these formulations remains the same.
Implantable Corticosteroids
Implantable Corticosteroids allow intraocular delivery of high concentration of medication, over a sustained period while avoiding systemic toxicity. This implants are preferred in patients with moderate to severe disease with recalcitrant macular edema and for whom systemic immunosuppression medications are contraindicated, intolerable, or inefficient to completely control inflammation. Essentially, two types of implants are available:
- Nonbiodegradable implants (e.g., fluocinolone acetonide intravitreal implant), which have to be replaced when their efficacy has expired, and
- Biodegradable implants (e.g., dexamethasone intravitreal implant).
Retisert: Fluocinolone Acetonide
In 2005, the FDA approved a nonbiodegradable intraocular sustained-release implant containing fluocinolone acetonide (Retisert, Bausch and Lomb, Rochester, NY) for use in the treatment of noninfectious intermediate, posterior, and panuveitis.[17] The implant is anchored at the pars plana surgically and designed to deliver 590 μg of fluocinolone acetonide into the vitreous over a 2–3-year period with minimal systemic absorption. The Multicenter Uveitis Steroid Treatment (MUST) trial was a randomized, comparative efficacy, clinical trial that compared the efficacy and safety of implant versus systemic treatments for severe forms of uveitis.[18] The study concluded that there was no significant difference in efficacy and but increased ocular complications when using the fluocinolone implant at 2 years. Over the 24-month period, implant assigned eyes had a higher risk of cataract surgery, treatment for elevated intraocular pressure, and glaucoma. Baseline visual field testing and optic nerve imaging are therefore recommended for patients undergoing fluocinolone implant surgery. The use of implants largely remains limited due to concerns about costs and complications.
Ozurdex: Dexamethasone Drug Delivery System (DDS)
Dexamethasone is five times more potent than triamcinolone acetonide, but has a short half-life in the eye. The rationale to develop a drug delivery system was to achieve a sustained concentration of the drug in the eye. Ozurdex is a sustained-release biodegradable intravitreal implant containing 0.7 mg dexamethasone in a solid polymer drug delivery system. As dexamethasone is released, the copolymer of lactic acid and glycolic acid slowing degrades into carbon dioxide and water. It enables dual-phase pharmacokinetics, initially releasing a burst of dexamethasone to rapidly achieve a therapeutic concentration, followed by a slower sustained release over 3 - 6 months. It is administered as an intravitreal injection using a 22-G applicator through the par plana under the sterile biplanar technique. The biodegradable design allows sequential implantation without the need for surgical removal. Ozurdex was approved by the US FDA in 2010 as first-line therapy in the treatment of macular edema associated with non-infectious intermediate and posterior uveitis.[19] A large prospective cohort study evaluated dexamethasone intravitreous drug delivery system in 315 patients with chronic CME of various origins and pointed out its efficacy and a lack of adverse effects.[20] With regards to safety, dexamethasone implant has a 50 % less chance of development of glaucoma and cataract progression with favorable visual outcomes.[21] These implants might become the preferred treatment for uveitis macular edema in the future.
Anti-VEGF
The use of intravitreal anti-VEGF therapies, bevacizumab and ranibizumab has recently been described as off-label treatment for inflammatory macular edema with active uveitis. Their efficacy is found to be variable, maybe because they do not possess anti-inflammatory properties. The effect has not been yet systematically investigated. Moreover, their length of effect is shorter than periocular or intravitreal steroids, but they are unlikely cause glaucoma or cataract progression.
Immunosuppressive:
In the long-term treatment of macular edema, corticosteroid-sparing agents are preferred to avoid the side effects of corticosteroids. The antimetabolites methotrexate, azathioprine, mycophenolate mofetil, and T-cell inhibitors like cyclosporine act primarily as an anti-inflammatory agent and are therefore beneficial for macular edema. Mycophenolate mofetil proved to be safe and very effective in controlling macular edema and in reducing the uveitis relapse rate.[22] A retrospective series showed intravitreal methotrexate therapy in active uveitis or uveitic CME to result in remission for around 10-30 months with single or two injections, in addition to reduction in steroid doses.[23] It is found to decrease aqueous humor levels of IL-6 and IL-8 in treatment eyes.[24] Intravitreal methotrexate may be a reasonable and effective option for patients with active unilateral uveitis and/or inflammatory CME who are known steroid responders.
Biologics
Biologics have been tried in recalcitrant cases of inflammatory macular edema. Anti-TNFα agents offer a more targeted suppression of immune effector responses. Three anti- TNFs agents are currently available for clinical use: etanercept, infliximab, and adalimumab. The safety of biologics, especially in long-term use, remains undetermined due to risks of various infections, the development of autoimmune and demyelinating diseases, the occurrence of malignancies, and congestive heart failure. Their efficacy and safety are yet to be investigated for use in inflammatory macular edema, nevertheless promising an exciting new frontier.
Carbonic Anhydrase Inhibitors & Somatostatin analogs
Carbonic anhydrase inhibitors reduce aqueous production and possible leakage from the RPE. They have no significant effect on visual acuity improvement and usually responsive to young individuals. [25,26] Systemic administration of acetazolamide has a little role in uveitic macular edema in the absence of active inflammation. [27] With its adverse effect profile of nausea, drowsiness, fatigue, paraesthesia, metabolic acidosis, and urolithiasis; using them as long term agents is not beneficial.
Somatostatin analogs such as octreotide blocks the local and systemic production of growth hormone, insulin-like growth factor and VEGF, which are all associated with angiogenesis and endothelial cell proliferation and stabilize the BRB. It has been found effective in inflammatory edema. [28]
|
Table 4: Factors to consider prior to initiating therapy and Pearls to management |
|
|
Laterality |
Unilateral: local therapy; Bilateral: systemic therapy preferred |
|
Lens status |
Pseudophakia with normal IOP: topical or periocular steroids Phakic- counsel for risk of cataract progression |
|
Refractory cases or Steroid responders |
Consider alternate therapy (Immunosuppressive, Biologics) |
|
Immunocompromised patients |
Avoid systemic immunosuppression. Consider steroid implant. |
|
Infectious etiology |
Treat the infection (Anti-protozoal agents, Anti-virals) |
|
Patient Age |
Risk of glaucoma and cataract development high with topical and local steroid therapy. Monitor IOP and optic disc health. Consider alternate therapy, if signs of glaucoma observed. |
|
Structural abnormalities (ERM, VMT) |
May require surgery |
Surgical Management: Primary Vitrectomy
Theoretically, vitrectomy removes the inflammatory mediators contained within the vitreous while prospectively reducing the time inflammatory factors retained within the vitreous cavity. In addition, mechanical traction following the formation of epiretinal membranes, and subsequently macular edema, is a known factor for medical treatment failure, where vitrectomy offers a better hand. In 1992, Kaplan suggested that vitrectomy may provide an alternative to systemic immunosuppression in intermediate uveitis. [29] Since then, intermediate uveitis has been the most common indication of vitrectomy for uveitis, with generally positive results for both macular edema and vision. Also in pediatric uveitis, par plana vitrectomy might improve macular edema and lead to a decrease of systemic immunosuppressive therapies. The data is not convincing for functional improvement, but also the modality has not been adequately studied as a treatment for uveitic macular edema at present.
Conclusion
The evolving knowledge on the pathophysiology of inflammatory macular edema will promise new avenues in diagnostic and therapeutic modalities. The priority in treatment is to reduce inflammatory activity aggressively, being mindful of the permanent structural changes with long-standing ME. The precise indications and treatment strategies for inflammatory ME are yet to be delineated. But the modern treatment is mainly through immunosuppression with steroid therapy. Dexamethasone implants represent the most promising long acing steroid-based option. Newer treatments await experience and evidence.
Reference:
- Rothova A, Suttorp-van Schlten MSA, Treffers WF, Kijlstra A. Causes and frequency of blindness in patients with intraocular inflammatory disease. Br J Ophthalmol. 1996;80(4): 332–6.
- Lardenoye CW, van Kooij B, Rothova A. Impact of macular edema on visual acuity in uveitis. Ophthalmology 2006; 113:1446–1449.
- Rothova A. Inflammatory cystoid macular edema. Curr Opin Ophthalmol 2007, 18:487–492.
- van Kooij B, Probst K, Fijnheer R, et al. Risk factors for cystoid macular edema in patients with uveitis. Eye (Lond) 2008;22:256–260.
- van Kooij B, Fijnheer R, Roest M, Rothova A. Trace microalbuminuria in inflammatory cystoid macular edema. Am J Ophthalmol 2004; 138:1010–1015.
- Johnson MW. Etiology and treatment of macular edema. Am J Ophthalmol. 2009;147(1):11–21.
- Fine HF, Baffi J, Reed GF, et al. Aqueous humor and plasma vascular endothelial growth factor in uveitis-associated cystoid macular edema. Am J Ophthalmol 2001; 132:794–796.
- van Kooij B, Rothova A, Rijkers GT, de Groot-Mijnes JD. Distinct cytokine and chemokine profiles in the aqueous of patients with uveitis and cystoid macular edema. Am J Ophthalmol 2006; 142:192–194.
- Schaal S, Kaplan HJ, editors. Cystoid Macular Edema: Medical and Surgical Management. Springer; 2016 Dec 29.
- Kiss CG, Barisani-Asenbauer T, Maca S, et al. Reading performance of patients with uveitis-associated cystoid macular edema. Am J Ophthalmol 2006; 142:620–624.
- Rothova A. Inflammatory cystoid macular edema. Current Opinion in Ophthalmology. 2007 Nov 1;18(6):487-92.
- Allegri P, Murialdo U, Peri S, Carniglia R, Crivelli MG, Compiano S, Autuori S, Mastromarino A, Zurria M, Marrazzo G. Randomized, double-blind, placebo-controlled clinical trial on the efficacy of 0.5% indomethacin eye drops in uveitic macular edema. Invest Ophthalmol Vis Sci. 2014;55(3):1463–70.
- Radwan AE, Arcinue CA, Yang P, Artornsombudh P, Abu Al-Fadl EM, Foster CS. Bromfenac alone or with single intravitreal injection of bevacizumab or triamcinolone acetonide for treatment of uveitic macular edema. Graefes Arch Clin Exp Ophthalmol. 2013;251:1801–6.
- Biswas J, Majumder PD, editors. Uveitis: An Update. Springer; 2015 Nov 13.
- Nozik RA. Periocular injection of steroids. Trans Am Acad Ophthalmol Otolaryngol. 1972;76:695–705.
- Jonas, J.B., Effects of triamcinolone acetonide injections with and without preservative.Br J Ophthalmol.2007;91(9):p.1099-101.
- Brumm MV, Nguyen QD. Fluocinolone acetonide intravitreal sustained release device-a new addition to the armamentarium of uveitic management. Int J Nanomedicine. 2007;2(1): 55–64.
- Kempen JH, Altaweel MM, Holbrook JT, Jabs DA, Louis TA, Sugar EA, Thorne JE, Multicenter Uveitis Steroid Treatment (MUST) Trial Research Group, Writing Committee. Randomized comparison of systemic anti-inflammatory therapy versus fluocinolone acetonide implant for intermediate, posterior, and panuveitis: the multicenter uveitis steroid treatment trial. Ophthalmology. 2011 Oct 31;118(10):1916-26.
- Hunter RS, Lobo AM. Dexamethasone intravitreal implant for the treatment of noninfectious uveitis. Clin Ophthalmol. 2011;5:1613–21.
- Kuppermann BD, Blumenkranz MS, Haller JA, et al., Dexamethasone DDS phase II study group. Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch Ophthalmol 2007; 125:309–317.
- Arcinue CA, Ceron OM, Foster CS. A comparison between the fluocinolone acetonide (Retisert) and dexamethasone (Ozurdex) intravitreal implants in uveitis. J Ocul Pharmacol Ther. 2013;29:501–7.
- Neri P, Mariotti C, Cimino L, Mercanti L, Giovannini A. Longterm control of cystoid macular oedema in noninfectious uveitis with Mycophenolate Mofetil. Int Ophthalmol. 2009;29:127–33.
- Taylor SRJ, Banker A, Schlaen A, Couto C, Matthe E, Joshi L, Menezo V, Nguyen E, Tokinsnetzer O, Bar A, Morarji J, McCluskey P, Lightman S. Intraocular methotrexate can induce extended remission in some patients in noninfectious uveitis. Retina. 2013;33(10):2149–54.
- Bea JH, Lee SC. Effect of intravitreal methotrexate and aqueous humor cytokine levels in refractory retinal vasculitis in Behcet disease. Retina. 2012;32(7):1395–402.
- Whitcup SM, Csaky KG, Podgor MJ, Chew EY, Perry CH, Nussenblatt RB. A randomised, masked, cross-over trial of acetazolamide for cystoid macular edema in patients with uveitis. Ophthalmology 1996;103:1054–62.
- Farber MD, Lam S, Tessler HH, Jennings TJ, Cross A, Rusin MM. Reduction of macular oedema by acetazolamide in patients with chronic iridocyclitis: a randomised prospective crossover study. Br J Ophthalmol. 1994;78:4–7.
- Schilling H, Heiligenhaus A, Laube T, et al. Long-term effect of acetazolamide treatment of patients with uveitic chronic cystoid macular edema is limited by persisting inflammation. Retin a 2005;25(2) :182–188.
- Misotten T, Van Laar JAM, Van der Loos Tl, et al. Octreotide long-acting repeatable for the treatment of chronic macular edema in uveitis. Am J Ophthalmol. 2007;144:838–843.
- Kaplan H. Surgical treatment of intermediate uveitis. Dev Ophthalmol. 1992;23:185–9.