

Brief Scenario of The Case:
A 50-year-old male patient was seen on 27th January 2021 with a chief complainof sudden painful loss of vision in his right eye for 1 week after lifting a heavyweight object at work.
History of Present Illness:
The patient’s only complainwas a black spot and decreased vision in an otherwise normal right eye, which occurred after lifting a heavyweight object (100 kg) at work.
Past Ocular History:
The patientwas using glasses for near vision (+1.00DS) for both eyes.
Past Medical History:
The patient was a chronic tobacco chewer. He had no other significant medical history.
Family History:
No family history of hypertension, diabetes, any neurological disease, or coagulopathy condition.
Systemic Examination:
The patienthad a blood pressure of 120/80, RBS was 127 mg%, his Pulse rate was 78/min. His central nervous system, circulatory system, and respiratory system examinations were normal.
Ocular Examination:
1. Best-corrected visual acuity (Snellen)
• Right eye (OD)- 20/800
• Left eye (OS)- 20/20
2. Ocular motility was full and free in all gazes for both eyes.
3. Intraocular pressure on NCT
• OD- 14 mmHg
• OS- 16 mmHg
4. Pupil was circular, central, and reacting to light in both eyes. No evidence of RAPD.
5. Slit-lamp examination
• Lid and lashes- normal in both eyes
• Conjunctiva and scleral- normal in both eyes
• Cornea- clear in both eyes
• Anterior chamber- normal in-depth and quiet in both eyes
• Iris- normal in color and pattern in both eyes
• Lens- clear in both eyes
6. Dilated fundus examination (fig. 1)
Vitreousclear in both eyes
Disc normal in size, shape, color, and margins in both eyes
Macula
- OD- A large boat-shaped hemorrhage was present in the pre-macular area with obscuration of underlying vessels
- OS- normal
Vessels normal, dichotomous in both the eyes
Periphery No other lesion noted
Ancillary Investigations:

Fig. 1 Right eye fundus shows a well-circumscribed, large, dome-shaped hemorrhage in a pre-macular area extending up to the temporal margin of the disc.
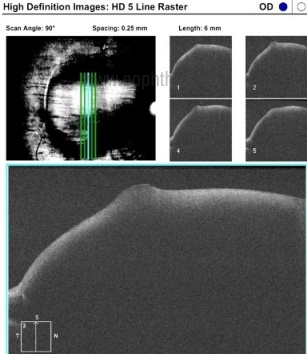
Fig. 2 OCT of the same eye showing large pre-macular hemorrhage with evident backshadowing.
Clinical Course of The Condition:
Since the time of presentation was more than a week and the color of the hemorrhage appeared dark red (indicating clotting of blood), Vitrectomy + ILM peeling was advised under local anesthesia explaining the pros and cons of the condition. The Post-op condition of the patient was quite stable. On 1-month follow-up, the best-corrected visual acuity in the right eye was 20/40. On fundus examination, the central fundus appeared clear, with a thin rim of residual blood seen around the arcades. (fig. 3).

Fig. 3 Fundus photo of the same eye on follow-up shows clear central fundus, with a rim of residual blood seen around the arcades.
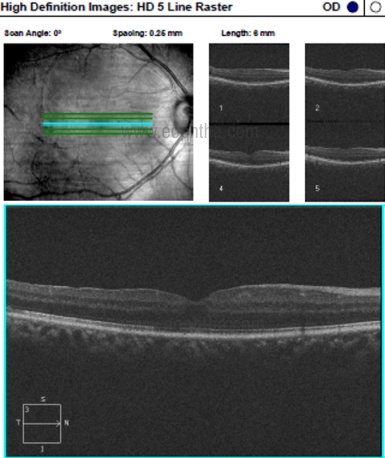
Fig. 4OCT of the same eye shows a completely resolved hemorrhage at the macula with a normal foveal contour.
Differential Diagnosis:
- Valsalva hemorrhagic retinopathy
- Sub-internal limiting membrane haemorrhage
- Sub-hyaloid haemorrhage
- Purtscher’s retinopathy
- Terson’s syndrome
- Hypertensive retinopathy
- Diabetic retinopathy
- Posterior vitreous detachment
Diagnosis:
Sub ILM hemorrhage secondary to Valsalva Retinopathy
Discussion:
Etiology/epidemiology
Premacular hemorrhage is a rare condition, may present as a uniocular or binocular disease. The most common cause being Valsalva retinopathy that occurs due to a sudden increase in intra-cavitary pressure under closed glottis or due to compressive injuries, which leads to retinal capillary bleed. Terson syndrome is associated with underlying intracranial bleeding that ultimately leads to increased intraocular pressure and hemorrhage. Other causes can be the formation of macroaneurysm in the retina that ruptured, blood coagulopathy, etc.
Pathophysiology
An increase in intraocular or intra-cavitary pressure leads to decreased venous return and increased venous pressure that transfers to retinal veins also and it increases the capillary rupture chances and eventually, hemorrhage occurs. In blood dyscrasia, due to decreased blood cells, coagulability decreases, and the integrity of retinal vessel endothelium is compromised. These processes lead to increased endothelial permeability and allow blood to extravasate. Due to blood, retinal pigment epithelium cells migrate even if the retina is intact. Moreover, heme and ferrous compounds present in the blood cause further toxicity to retinal cells and can cause proliferative changes in the retina. Due to retinal insult, glial cell proliferation may also occur that may cause further neurodegenerative changes in the retina and leads to the poor visual outcome even after treatment.
Clinical features
The patient can experience sudden diminished vision or acute loss of vision, visual field defects, complaints of floaters in an otherwise normal eye. On examination there occurs well-circumscribed retinal hemorrhage in the macular area with glistening reflexes and no underlying vessels visible.
Ancillary investigation
A thorough fundus examination should be done for any hemorrhage and associated peripheral retinal findings. On concluding premacular bleed, an OCT should be done to locate the exact site for bleed. Sub ILM and subhyaloid bleed can be tricky to diagnose on the OCT. The internal limiting membrane present over the hemorrhage is hyperreflective and the posterior hyaloid is seen as a hypo reflective band. The only confirmatory test is intraoperative staining and peeling of the membrane present over hemorrhage and its histopathological examination.
Laboratory investigations
Complete blood count, bleeding-clotting time, PT/INR for any coagulation disorder, blood pressure monitoring for hypertension, blood sugar levels for diabetes should be done to rule out related causes.
Treatment
- Observation: Treatment options for sub-ILM hemorrhage vary from just observation to surgical intervention depending on the size and duration of the bleed. Hemorrhage within 1 disc diameter size can spontaneously reabsorb in 2-3 weeks but larger size bleeds may take few months or need surgery later. Early intervention is helpful for a better outcome as it decreases the retinal toxicity due to long-standing heme.
- Nd: YAG laser is an option for intervention in fresh hemorrhage, but some complications can occur as the formation of epiretinal membrane, retinal detachment, etc.
- Intravitreal injection of tissue plasminogen activator (tPA) is helpful in dissolving the settled blood over the macula. It emphasizes the conversion of plasminogen to plasmin and plasmin acts as a fibrinolytic agent. Sometimes it is followed by pneumopexy with a 100 percentage of expansile concentration of gas (C3F8/SF6) thathelps in pushing the heme away from the center. After this procedure patient is instructed to be in the prone position.
- Vitrectomy with ILM peeling and aspiration of blood is the most definite intervention, especially when the hemorrhage is dense, large, or if spontaneous reabsorption has not occurred in 3-4 weeks. If done uneventfully, it can yield great results with rapid visual recovery. Complications can be in form of retinal detachment, cataract, increased intraocular pressure, etc.
Valsalva Retinopathy |
|
|
Etiology
|
Signs
|
|
Symptoms
|
Differentials
|
|
Investigations
|
Treatment
|