
Question
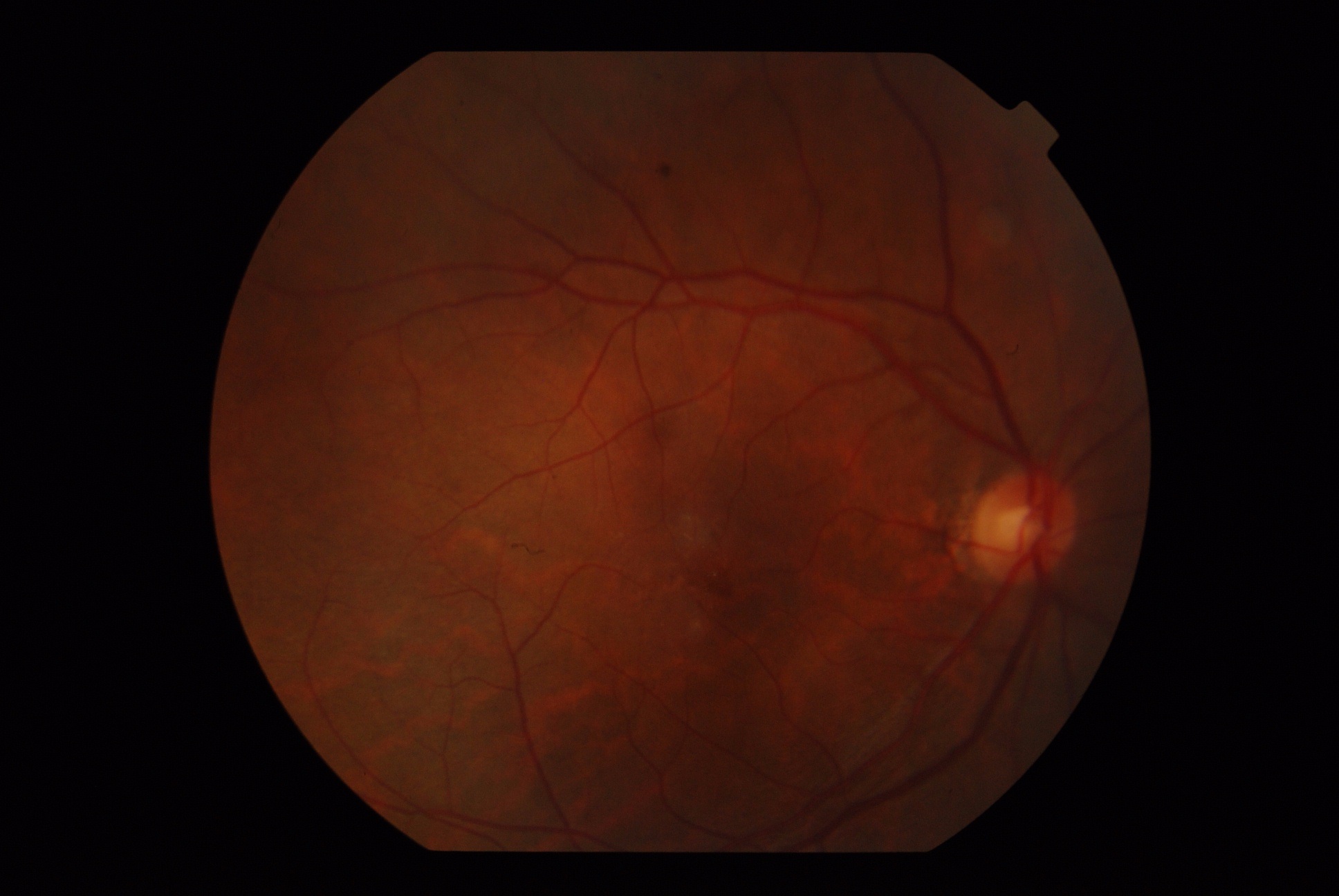
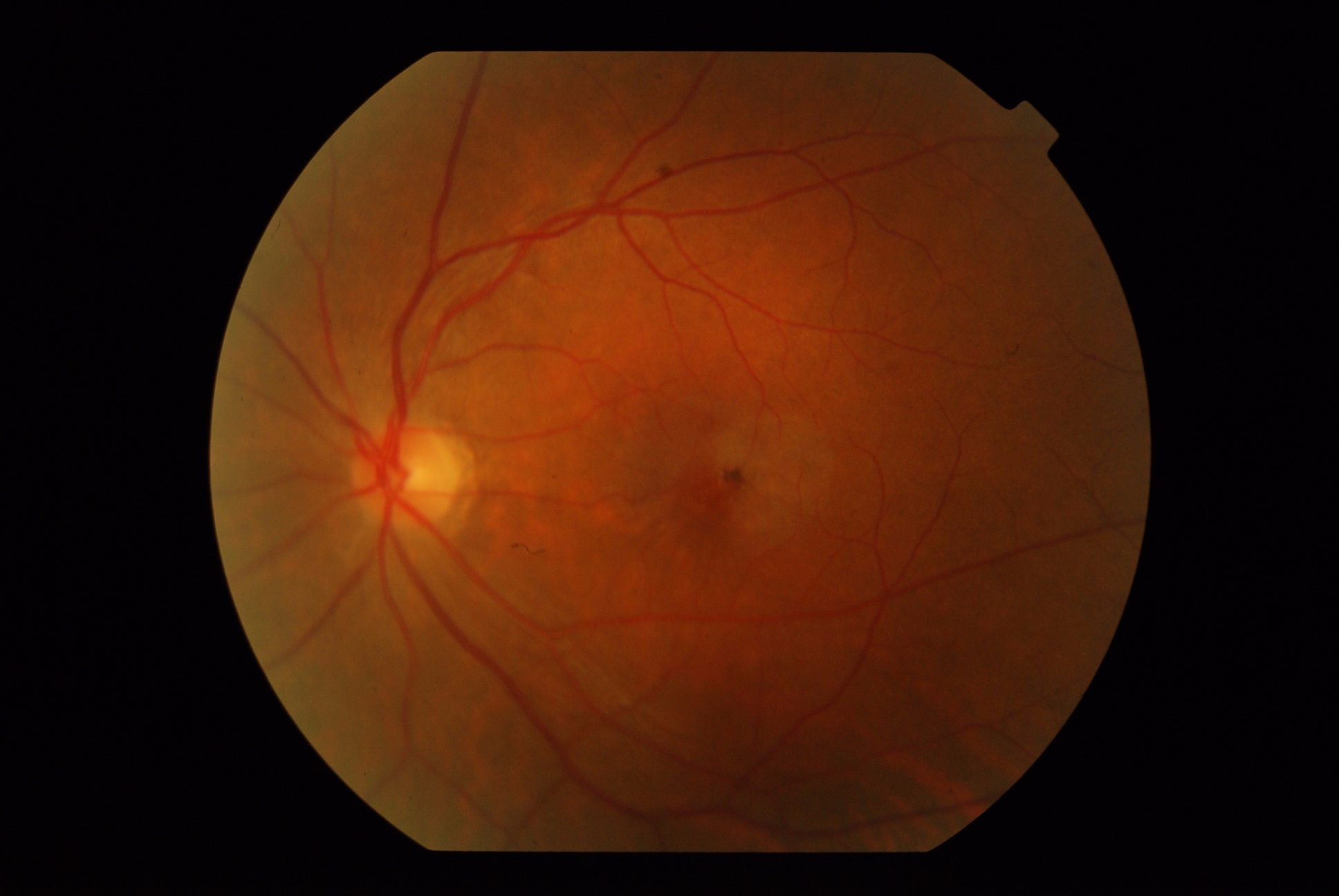
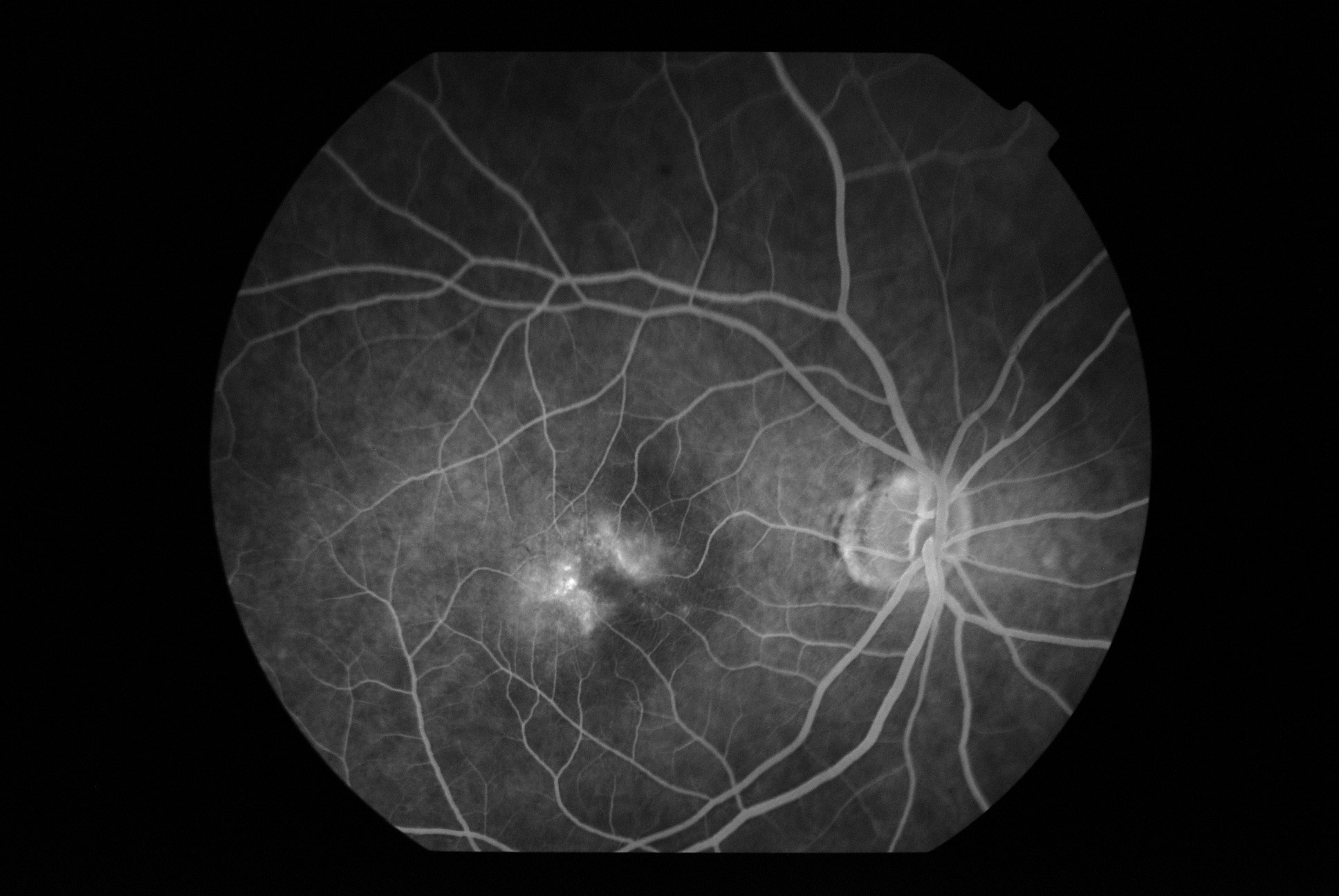
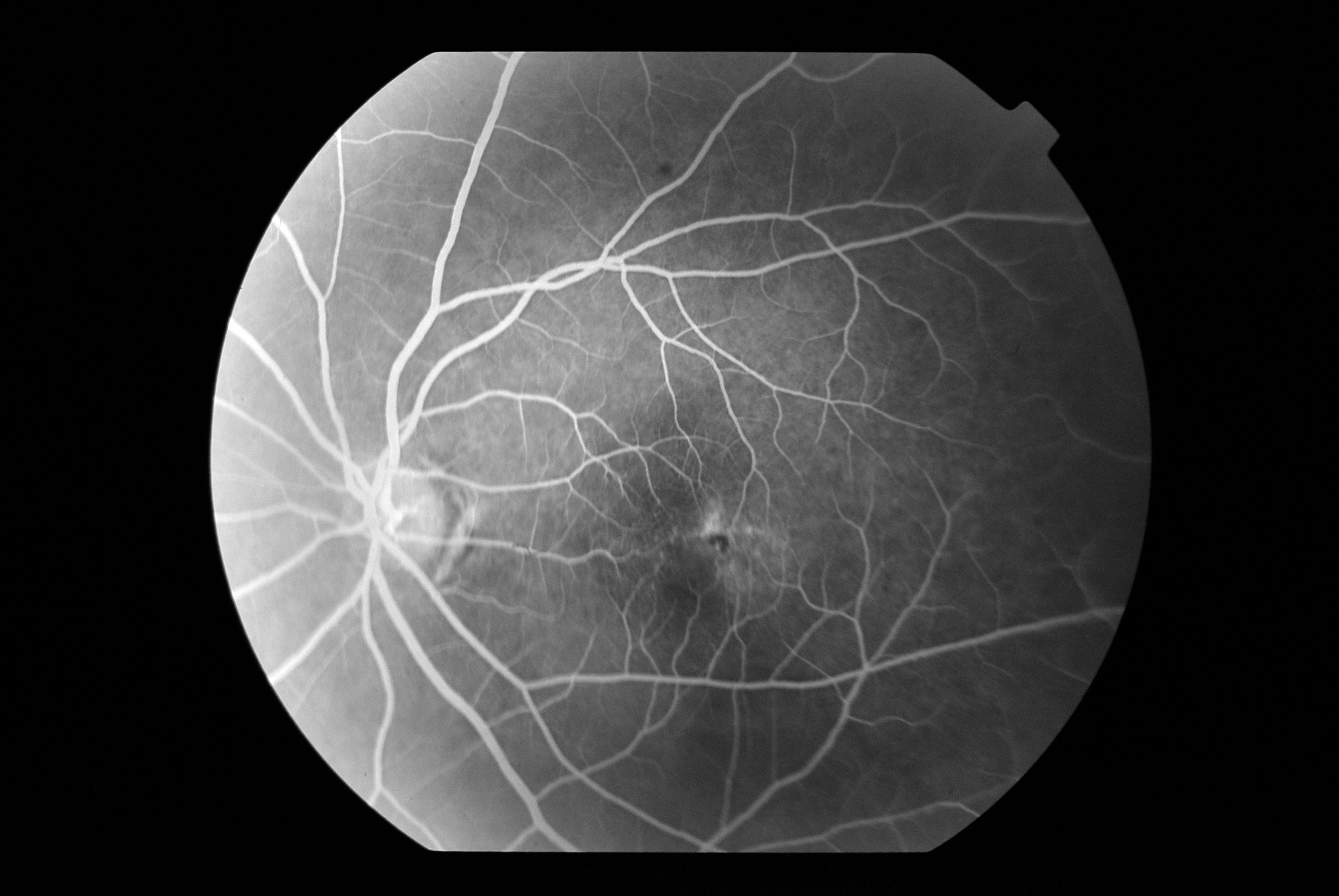
A 61-year-old presented with OU diminution of vision. He complains of distortion of letters which he has noticed in the last few months. He is a well-controlled diabetic for 13 years. There are no other systemic issues. Examination revealed a BCVA of OD 6/18(P) N8, OS 6/24 N8. The anterior segment is unremarkable except for pseudophakia OU (no e/o PCO). Fundus and FFA as shown
- What is the most probable diagnosis (give your differential)?
- Which other investigation will help in the diagnosis
- How will you treat the patient?
Answer:
Idiopathic Juxtafoveal Retinal Telangiectasia(IJRT)
Classification
COATS
- Subretinal exudation without vascular abnormalities
- Subretinal exudation with vascular abnormalities
- Exudation with AV malformation
This classification is mostly for interest and not followed anymore
GASS and BLODI ( 1993) This classification was a modification of the original Gass and Oyakawa classification of 1982
1A) Congenital in nature, having a UNILATERAL presentation in MALES
1B) Similar to above having a better prognosis and limited retinal abnormality
2A) Occult Non-exudative IJRT: This is the commonly known parafoveal telangiectasia and will be dealt with here
2B) Juvenile Occult familial IJRT
3A) Occlusive IJRT
3B) Occlusive IJRT with CNS vasculopathy
YANUZZI (Currently followed)
Type 1 Macular Telangiectasia: This was the original Gass type 1A and 1 B combined together
Type 2 Macular Telangiectasia: This the Gass type 2A
This is again divided into:
- Non-proliferative: without e/o CNVM
- Proliferative: having e/o CNVM
The original 2B and 3 of the Gass classification were omitted in view of their rarity
Type 2 is further divided into 5 stages
Stage1: Difficult to appreciate but the temporal parafoveal area has a greyish appearance with loss of transparency
Stage 2: The transparency increases with the appearance of telangiectatic vessels
Stage 3: Presence of right-angled venules
Stage 4: Presence of RPE hyperplasia
Stage 5: the presence of CNVM
The presence of intraretinal crystals can occur in any stage.
Salient Points about Macular Telangiectasia Type 2
The functional parameter most important for assessing the condition is not Visual acuity, but microperimetry. The earliest sign is the occurrence of greyish discoloration of the temporal fovea
Why: This is thought to occur secondary to nutritional and ischemic damage to the middle layers.
- The telangiectatic vessels are generally not associated with exudation until CNVM develops.
- The RPE clumps occur along the right-angled venules and are often thought to increase the chances of CNVM
Presence of Crystals: why???
- Formed by degenerating MULLER cells
- Retinal capillary telangiectasia surrounded by lipofuschin cells
- The presence of crystals does not correlate with the severity of the condition
- Located mostly in the inner retinal layers
FFA
- The classical FFA pattern is thought to be dilated ectatic capillaries that leak dye in the parafoveal area
- In the early stages of the disease, there are no dilated capillaries, only minimal staining.
- There is characteristic oval-shaped hyperfluorescence.
- The leakage is not related to any cystic spaces
OCT
- Outer retinal atrophy with outer retinal thinning and loss of architecture
- The occurrence of hyporeflective spaces, they can occur in the outer or inner retinal layers
- Presence of hyperreflective foci
- Presence of other features s/o CNVM
Fundus autofluorescence: It’s a newer modality of investigation which is supposed to be the most sensitive modality to verify IJRT in the initial stages
Other imaging modalities are:
- Adaptive optics
- Confocal reflectance imaging
- Microperimetry
Clinical signs suggestive of development of CNVM
- Sudden onset loss of vision
- Presence of subretinal hemorrhage
- Presence of exudation
- Cystoid edema
- Retinochoroidal anastomosis
In this case, since there are no signs of CNVM only a close watch is needed.There is no role of the laser at this stage.If and when any signs of CNVM appear anti-VEGF can be used with or without PDT.